
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
An unusual failed reverse shoulder arthroplasty: Case report
Mahircan Demir1* Ibrahim Faruk Adiguzel 2 Yusuf Bayram 3
1Zile State Hospital, Turkey.
2Ankara Etlik City Hospital, Turkey.
3Private Pendik Century Hospital, Turkey.
*Corresponding Author : Mahircan Demir
Zile State Hospital, Turkey.
Tel: +90-5358137964;
Email: mahir19911991@gmail.com
Received : Dec 15, 2020
Accepted : Dec 30, 2020
Published : Dec 31, 2020
Archived : www.jcimcr.org
Copyright : © Demir M (2023).
Abstract
Shoulder arthroplasty is a surgical method used to relieve pain and restore functionality in cases of primary and secondary degenerative joint diseases and post-traumatic proximal humeral fractures [1]. It is especially preferred in cases such as irreparable rotator cuff injuries, pseudoparalysis, multi-part proximal humerus fractures and degeneration secondary to rheumatoid arthritis [2]. Recently, shoulder arthroplasty applications have gained momentum. There are different types of partial, total and reverse shoulder prosthesis designs [3]. Various complications, such as dislocation, infection, loosening, scapula or acromion fractures and neuropraxia, may develop in relation to these shoulder prostheses [4]. In this article, a case of reverse shoulder prosthesis and an uncommon complication and treatment process are presented.
Citation: Mahircan Demir M, Adiguzel IF, Bayram Y. An unusual failed reverse shoulder arthroplasty: Case report. J Clin Images Med Case Rep. 2023; 4(3): 2352.
Introduction
Reverse shoulder prostheses were first designed by Paul Grammont in France in 1980 [5]. Today, their application and popularity are increasing worldwide. One study stated that there were 823,361 patients who underwent shoulder prosthesis in the USA in 2017 [6].
Reverse shoulder prosthesis is a surgical treatment used to relieve pain and restore functionality. Reverse shoulder prostheses have a more stable structure than normal shoulder prostheses. They increase the deltoid moment arm length by moving the centre of motion medially and inferiorly; thus, flexion and abduction movement of the shoulder is provided by the deltoid muscle [7].
Reverse shoulder prosthesis is preferred in cases such as multi-part humeral fractures, irreparable rotator cuff tears, pseudoparalysis, implant failures, sequelae of rheumatoid disease and post tumour resection. Advanced age, sufficient bone stock and a functional deltoid muscle are required for the prosthesis to be applied.
Intraoperative or postoperative events that affect a patient’s final outcome are considered complications [8]. Complication rates associated with primary reverse shoulder prostheses have been reported to vary between 3% and 24%. The most common complications leading to revision are loosening or dislocation, infection, periprostatic fracture and glenoid base plate loosening [9]. Glenoid and humeral component separation is very rare, and there are limited case reports [10]. Such complications have decreased due to advances in prosthesis designs.
Case report
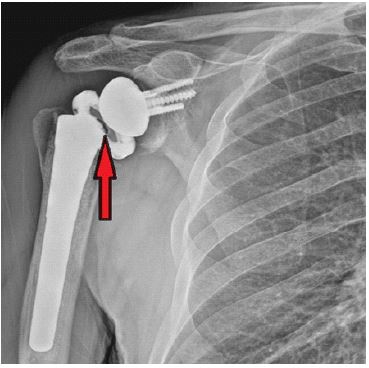
A 58-year-old male patient underwent right reverse shoulder arthroplasty (Tıpmed-medical RSS) at another centre due to a massive rotator cuff tear. The patient was admitted to our clinic with the complaint of shoulder pain in the ninth month postoperatively. There was no history of trauma or coercion. No signs of infection were observed at the incision site. The patient stated that he heard a sound from his shoulder while sleep and continued pain complaints afterwards. On physical examination, it was observed that shoulder movements were limited and painful. A mechanical jumping sound was heard with passive movements of the shoulder. It was observed that right shoulder abduction was 15 degrees, flexion was 30 degrees and the arm that could not externally rotate was in an internal rotation posture. A complete blood count and biochemistry tests were performed. There was no finding indicating infection. A direct radiograph revealed a gap between the humeral stem and the humeral tray.
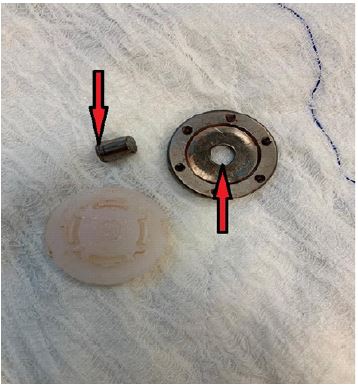
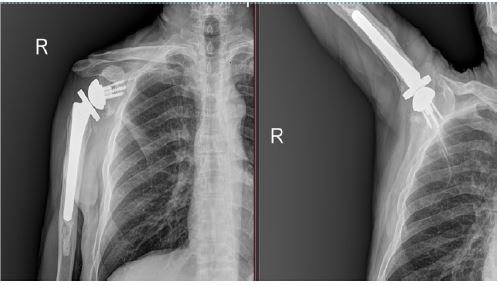
After the evaluations, it was decided to perform revision surgery. The prosthesis was reached via the deltopectoral incision made during the patient’s previous operation. It was observed that the junction point between the humeral tray and the humeral stem was broken. Afterwards, the fractured part on the humeral stem side was removed by means of an osteotome, and the shoulder prosthesis was revised by placing a new humeral tray.

Discussion
Reverse shoulder prostheses are designed to treat irreparable rotator cuff tears but have now become ideal optionsto treat proximal humeral fractures, tumour resections, arthritis with or without rheumatologic conditions, chronic dislocations and partial or total shoulder prosthesis failures [11].
Complications associated with reverse shoulder prostheses include infection, dislocation, intraoperative fractures, post-operative fractures, aseptic loosening, glenoid screw problems, hematoma, vascular nerve injuries, notching of the scapula, heterotopic ossification and cement extravasation. Some authors argue that complications affect the final result, while others argue the opposite. Obviously, the definition of complications varies. Complications can be defined as intraoperative and postoperative events that negatively affect the final result.
Complication rates reported for reverse shoulder prosthesis vary. These differences are due to the indication, the prosthesis design and the experience of the surgeon. In a study by Wall et al., the complication rate was found to be 13% for primary cases and 37% for revision cases. Wierks et al. reported 33 complications in 15 patients, with the most frequently reported complications being neuropathy, intraoperative fractures and dislocations. Dislocations have been reported as the primary reason for revision surgery [11].
In our review of the literature, we did not find any cases similar to the one discussed here where the connection between the humeral tray and the humeral stem was broken. We believe the main problem is a manufacturing defect at the junction between the humeral tray and the humeral stem. A similar scenario could occur as a result of trauma.
During examinations requested by the patient in the preoperative period, we noticed that there was no connection between the humeral stem and the tray upon direct X-ray. The presence of passive shoulder movements, a metallic jumping sound and limited movement helped us decide on surgical treatment.
The fractured fragment was removed from the humeral stem by means of an osteotome. However, in situations where this might not be possible, humeral stem replacement might be necessary. This could lead to clinical conditions such as prolongation of the surgical time, prolongation of the recovery period, a negative final result and infection.
Conclusion
Fracture of the junction between the humeral tray and the humeral stem is a condition that can cause pain and limited movement. It is a challenging situation for surgeons, as they cannot give a clear diagnosis when imaging is not performed at the appropriate angle. The rare complication we encountered should be kept in mind for patients with sudden shoulder pain and limited motion after reverse shoulder prosthesis.
References
- Westermann RW, Pugely AJ, Martin CT, Gao Y, Wolf BR, Hettrich CMet al. Reverse shoulder arthroplasty in the United States: Aa comparison of national volume, patient demographics, complications, and surgical indications. The Iowa Orthopaedic Journal. 2015; 35: 41.
- Rugg CM, Coughlan MJ, Lansdown DA. Reverse total shoulder arthroplasty: Bbiomechanics and indications. Current Reviews in Musculoskeletal Medicine. 2019 Dec; 12(4): 542-553.
- Hatzidakis AM, Norris TR, Boileau P. Reverse shoulder arthroplasty indications, technique, and results. Techniques in Shoulder & Elbow Surgery. 2005 Sep 1; 6(3): 135-149.
- Groh GI, Groh GM. Complications rates, reoperation rates, and the learning curve in reverse shoulder arthroplasty. Journal of Shoulder and Elbow Surgery. 2014 Mar 1; 23(3): 388-394.
- Krukenberg A, Imiolczyk JP, Moroder P, Scheibel M. Shoulder arthroplasty. Zeitschrift fur Orthopadie und Unfallchirurgie. 2018 Apr 17; 156(2): 227-238.
- Farley KX, Wilson JM, Kumar A, Gottschalk MB, Daly C, Sanchez-Sotelo J, Wagner ER. et al. Prevalence of shoulder arthroplasty in the United States and the increasing burden of revision shoulder arthroplasty. JBJS Open Access. 2021 Jul; 6.(3)
- Walker M, Brooks J, Willis M, Frankle M. How reverse shoulder arthroplasty works. Clinical Orthopaedics and Related Research®. 2011 Sep; 469(9): 2440-251.
- Zumstein MA, Pinedo M, Old J, Boileau P. Problems, complications, reoperations, and revisions in reverse total shoulder arthroplasty: Aa systematic review. J Shoulder Elbow Surg.2011; 20: 146-157.
- Alexander R. Markes, Edward Cheung, C. Benjamin Ma. Failed reverse shoulder arthroplasty and recommendations for revision.Current Reviews in Musculoskeletal Medicine. 2020; 13: 1-10.
- Stephens BC, Simon P, Clark RE, et al. Revision for a failed reverse: a 12-year review of a lateralized implant. J Shoulder Elbow Surg. 2016; 25: e115-e124.
- Barco R, Savvidou OD, Sperling JW, Sanchez-Sotelo J, Cofield RH, et al. . Complications in reverse shoulder arthroplasty. EFORT Open Reviews. 2016 Mar 30; 1(3): 72-80.