
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Schwannoma of the lateral aspect of the internal carotid
plexus: A case report and literature review
Rodrigo Mourão¹*; Nina Ventura²,³; Raquel Bezerra³; Bernardo Muniz³; Felipe Pinto4; Luany Ponce4
1Department of Radiology, Antonio Pedro Universitary Hospital (HUAP), Niteroi, RJ, Brazil.
2Department of Radiology, Clementino Fraga Filho Universitary Hospital (HUCFF), Rio de Janeiro, RJ, Brazil.
3Departmentof of Radiology, Paulo Niemeyer State Brain Institute (IECPN), Rio de Janeiro, RJ, Brazil.
4Department of Radiology, Medical School, Federal University of Rio de Janeiro (UFRJ), RJ, Brazil.
*Corresponding Author : Mourao Rodrigo
20 Senador Soares St., Vila Isabel, Rio de Janeiro, RJ, 20541-020, Brazil.
Ph: +55 21 993490669;
Email: rodrigomouraosilva@yahoo.com.br
ORCID ID: 0000-0001-7605-7597
Received : Feb 02, 2023
Accepted : Mar 27, 2023
Published : Apr 03, 2023
Archived : www.jcimcr.org
Copyright : © Rodrigo M (2023).
Abstract
Background: Schwannoma of the lateral aspect of the Internal Carotid Plexus (ICP) is an unusual tumor, defined through its relationship with the Internal Carotid Artery (ICA). In literature, only 3 are certainly originated from this portion of that plexus.
Methods: A 13-year-old male presented with 5 months of Peripheral Facial Paralysis (PFP) and hearing loss on the right. Imaging revelated a tumor in petrous apex, with infero-medial displacement of the petrous segment of the ICA. Biopsy revealed schwannoma.
Results: The patient was taken up for surgery, however the tumor adherence made complete resection impossible. After surgery, there was no clinical improvement.
Conclusions: Schwannoma of the lateral aspect of the ICP occurs from 13 to 35 years old, imaging exams do not differ from those in other locations, and surgery was favorable in only 1 case. We describe the youngest patient with this condition and the only one with PFP.
Citation: Mourão R, Ventura N, Bezerra R, Muniz B, Pinto F, Ponce L, et al. Schwannoma of the lateral aspect of the internal carotid plexus: A case report and literature review. J Clin Images Med Case Rep. 2023; 4(4): 2353.
Introduction
Schwannomas are commonly benign, solitary and slow-growing tumors from the Schwann cells, originated from myelinated peripheral, cranial or autonomic nerves [1-3]. They present variable internal cellular organization, with compact (Antoni A) and loose (Antoni B) areas, which influence their signal intensity on Magnetic Resonance Imaging (MRI) [1,4].
This tumor occur predominantly between the fourth and sixth decades, but can appear at any age [3], and represent about 8% of primary intracranial tumors, originating in 80-90% of the cases in the vestibulocochlear nerve [1,2,5]. They are rarely malignant or multiples, and, in these cases, frequently related to neurofibromatosis type I or II [3]. When associated with these phakomatosis it occurs around the second decade of life [3].
Cross section imaging shows well defined mass, remodelling bone structures, and deforming/displacing adjacent tissues. CT scan demonstrates soft tissue lesion with variable enhancement frequently vivid, may present calcifications and cystic degeneration. On MRI they are usually heterogeneous, hyperintense or hypointense on T2 and isointense or hypointense on T1, with homogeneous or heterogeneous enhancement after gadolinium [1,3,4,6]. The signal variation on T2 weighted imaging corresponds to the cellular organization of the tumor, where Antoni B regions show high signal and Antoni Alow signal, as well as the presence of cysts, calcifications and hemosiderin deposits [1,4]. There is no restriction on diffusion weighted images [4].
Case report
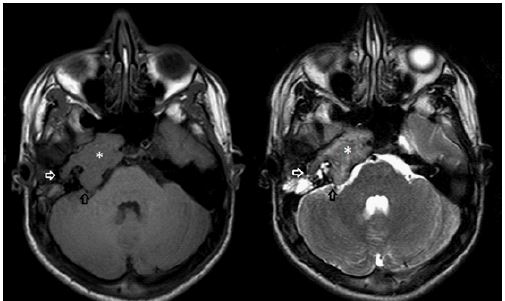
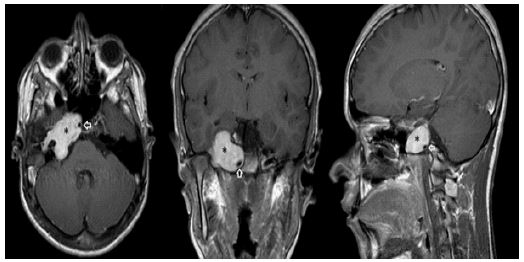
A 13-year-old male patient, without significant personal or family medical history, started with right sided peripheral facial paralysis for five months associated with sporadic episodes of vertigo. Later, he developed occasional headache and hearing loss on the same side. MRI of the brain showed an expansive lesion in the petrous bone with extension into the tympanic cavity and internal auditory canal, presenting an intermediate signal on T1, heterogeneous low signal on T2 and intense enhancement after gadolinium administration, without diffusion restriction.
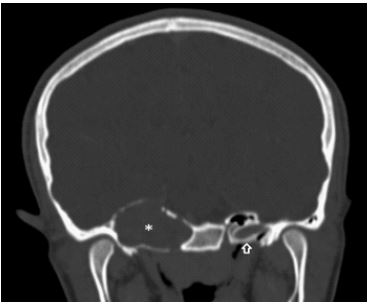
The lesion followed the Internal Carotid Artery (ICA) in cervical segment and vertical portion of petrous segment posteriorly, in horizontal portion inside carotid canal supero-laterally and in lacerum segment laterally, promoting infero-medial displacement of the petrous segment of ICA. The facial and vestibulocochlear nerves were compressed, but the trigeminal nerve and cavernous sinus were preserved. The Computed Tomography (CT) demonstrated a soft tissue mass with intense enhancement, without calcification, expanding the carotid canal. Schwannoma with predominant Antoni A areas was confirmed histologically after resection.
The patient’s age, its progressive symptoms and the tumor size, which contraindicated radiosurgery, led to the choice of surgical resection. However, tumor adherence to the internal carotid artery made complete resection of the neoplasm impossible. After surgery, there was no improvement in peripheral facial paralysis or of the hearing loss, and the patient was directed to radiotherapy.
Discussion
Schwannomas of the petrous apex/cavernous sinus are most common related to trigeminal nerves and rarely to oculomotor, trochlear, abducens, lesser or greater superficial petrosal nerves [2-6]. However, these nerves may not be the primary sites of this tumor, receiving different denominations in the literature such asintraosseous [4,6,7], primary [8] or sympathetic/internal carotid plexus Schwannomas [2,3,5,9].
The carotid plexus is a sympathetic plexus composed of postganglionic fibers derived from internal carotid nerve, a branch of the superior cervical ganglion [2,3]. It is situated in adventitia of the internal carotid artery and is divided into two plexuses: A larger lateral named internal carotid plexus and another smaller medial denominated cavernous plexus [2,3,9].
The internal carotid plexus has two segments, the first, inside the carotid canal giving rise to the deep petrosal and caroticotympanic nerves and, the second, inside the cavernous sinus that may send filaments, via abducens nerve, to the trigeminal nerve and the ciliary ganglion. The deep petrosal nerve joins the greater petrosal nerve to form the vidian nerve, which sends fibers to the sphenopalatine ganglion, and the caroticotympanic nerves originate the tympanic plexus. On the other hand, the cavernous plexus gives branches to cranial nerves II, III, IV, VI and to the ciliary ganglion [2,3,9].
The first to describe schwannomas in petrous apex was Solodnik [7] in 1986. At that time, he didn’t know its real origin, but believed that the tumor could originate from a small sympathetic or parasympathetic nerve. Horn [8] in 1995 related two cases of the schwannomas of the petrous apex, considering that the carotid nerve or periarterial sympathetic plexus branches were the most likely source to these neoplasms.
In another case report, Ture [2] in 2002 described a schwannoma of the medial part of the internal carotid plexus situated within the cavernous sinus, displacing the internal carotid artery supero-laterally, what would suggest its origin in the medial aspect of the internal carotid plexus. More recently, Takase [5] in 2016, describes one more case and suggests that the determination of the direction of ICA displacement may help establish the origin of schwannoma.
Besides these cases, few others have been described: Hamilton [3] and Gouiney [6], in 2011; Tamura [4], in 2015 and Goudihalli [9] in 2018 (See table 1, below). Of all the reports, only three have unquestionably tumors positioned superior and laterally to the internal carotid artery, suggesting an origin in the lateral portion of the internal carotid plexus. Therefore, we present the fourth petrous schwannoma with this origin and the younger patient described.
Interestingly, analyzing table 1, we see that of the 4 cases of schwannoma on the lateral aspect of the internal carotid plexus (cases 2, 3, 11 and 13), all presented hearing impairment and only one peripheral facial paralysis. Besides that, all of these cases have undergone surgery, three with unfavorable results, although radiosurgery, radiotherapy or combination of these may also be used in treatment.
Resume
Selection: The case comes from a referral hospital for surgical neurological treatments in the State of Rio de Janeiro, whose patient is still being monitored.
Justification: Through this case report, we expose the anatomy and clinical findings of a lesion in the temporal region, as well as relating the neurological, radiological, oncological and surgical aspects involved to the condition. In other words, it is a case that involves multiple fields of knowledge.
Clinical practice: With our case, we remind physicians, radiologists, neurologists, ENTs, surgeons, radiotherapists and oncologists that schwannoma can also appear primarily in the temporal region. In addition, we expanded the knowledge about this neoplasia, presenting the newest patient with tumor in that location and the only one to present with peripheral facial paralysis. We also demonstrate that the radiological findings of the primary lesion in this location are not different from those in other locations, and finally, we warn of the possibility of other non-surgical treatments, which should be considered in the next new cases, perhaps with even better results.
Table 1: The course of endoscopic treatments.
| DENOMINATION | AGE | SEX | SYMPTOMS | IMAGING | LOCALIZATION | CAROTID RELATION | LOCALIZATION | ||
|---|---|---|---|---|---|---|---|---|---|
| SOLODNIK, 1986 | INTRAOSSEOUS | 59 | MAN | HEADACHES TINNITUS AND HEARING LOSS UNSTEADINESS GAIT VEERED TO THE LEFT | EXPANSIVE WITH HOMOGENEOUS ENHANCEMENT | NOT ANALYZED | MEDIAL TO THE ICA | PETROUS APEX | |
| HORN, 1995 (CASE 1) | PRIMARY | 46 | WOMAN | AURAL FULLNESS MIDDLE EAR MASS | SMOOTH EROSION, ENLARGEMENT OF THE CAROTID CANAL, HOMOGENEOUS ENHANCEMENT SURROUND PARTIALLY PETROUS CAROTID ARTERY FROM CAROTID FORAMEN TO THE CAVERNOUS SINUS. | CAROTID CANAL AND CAVERNOUS SINUS | LATERAL TO THE ICA | 1 | PETROUS APEX |
| HORN, 1995 (CASE 2) | PRIMARY | 52 | MAN | HEARING LOSS EAR EFFUSION | EROSION, CT NONENHANCING AND T1 ENHANCING T2 HETEROGENEOUS SURROUND 2/3 PETROUS CAROTID ARTERY | CAROTID CANAL WITH CAVERNOUS SINUS FREE | SUPERO-LATERAL TO THE ICA | 2 | PETROUS APEX |
| TURE, 2002 | INTERNAL CAROTID PLEXUS | 29 | MAN | DOUBLE VISION | EROSION IN THE FLOOR CAVERNOUS SINUS T1 ISOINTENSE WITH HOMOGENEOUS ENHANCEMENT | CAVERNOUS SINUS WITH CAROTID CANAL FREE | INFEROMEDIAL TO THE ICA / ICA DISPLACED SUPERO-LATERALLY | CAVERNOUS SINUS | |
| HAMILTON, 2011 (CASE 1) | INTERNAL CAROTID PLEXUS | 27 | WOMAN | HEARING LOSS EAR EFFUSION HEADACHE, DIPLOPIA, ABDUCENS PALSY | EXPANSIVE, T1 ISOINTENSE WITH HOMOGENEOUS ENHANCEMENT T2 HYPOINTENSE HETEROGENEOUS, EUSTACHIAN TUBE BLOCKED EXTENSION TO CAVERNOUS SINUS AND INFERIORLLY | CAROTID CANAL AND CAVERNOUS SINUS | OCCLUSION, (Lateral position of the tumor cannot be confirmed) | duv | CAROTID CANAL |
| HAMILTON, 2011 (CASE 2) SEM CONFIRMAÇÃO | INTERNAL CAROTID PLEXUS | 68 | MAN | DIPLOPIA, ABDUCENS PALSY TINNITUS NASAL OBSTRUCTION HEADACHE | SMOOTH ESPANSIVE T1 ISOINTENSE WITH HOMOGENEOUS ENHANCEMENT, T2 HYPERINTENSE HOMOGENEOUS | CAROTID CANAL AND CAVERNOUS SINUS | ANTERO-MEDIAL TO THE ICA (BILATERAL?) | CAROTID CANAL | |
| GOINEY, 2011 | INTRAOSSEOUS | 48 | WOMAN | MIGRANES HEADACHE FACIAL HYPOESTHESIA | EXPANSIVE SMOOTHLY MARGINATED T1 ISOINTENSE WITH HOMOGENEOUS ENHANCEMENT T2 HYPERINTENSE HOMOGENEOUS WHITOUT RESTRICTED DIFFUSION | ? | ? | PETROUS APEX | |
| TAMURA, 2015 | INTRAOSSEOUS | 47 | MAN | DOUBLE VISION ABDUCENS PALSY | EXPANSIVE, ISODENSE WITHOUT CALCIFICATIONS T1 HYPOINTENSE WITH HETEROGENEOUS ENHANCEMENT T2 HYPERINTENSE HETEROGENEOUS AND DWI | CAROTID CANAL | MEDIAL TO THE ICA / ICA DISPLACED LATERALLY | PETROUS APEX | |
| TAKASE, 2016 | INTERNAL CAROTID PLEXUS | 54 | MAN | EAR FULLNESS DIPLOPIA | EROSION, DESTRUCTED CAROTID CANAL, ISODENSE WITHOUT CALCIFICATIONS HOMOGENEOUS ENHANCEMENT T2 HYPOINTENSE HETEROGENEOUS | CAROTID CANAL AND CAVERNOUS SINUS | INFERO-MEDIAL TO THE ICA/ ICA DISPLACED SUPERO-LATERALLY | PETROUS APEX | |
| GOUDIHALLI, 2018 (CASE 1) | INTERNAL CAROTID PLEXUS | 50 | MAN | HEARING LOSS CHRONIC OTITIS MEDIA | EXPANSIVE, HOMOGENEOUS ENHANCEMENT EUSTACHIAN TUBE BLOCKED EXTENDED INTO THE PARAPHARYNGEAL SPACE | CAROTID CANAL WITH CAVERNOUS SINUS FREE | SUPERO-LATERAL TO THE ICA / ICA DISPLACED INFERO-MEDIALLY | 3 | PETROUS APEX |
| GOUDIHALLI, 2018 (CASE 2) | INTERNAL CAROTID PLEXUS | 49 | WOMAN | EAR FULLNESS DIPLOPIA ABDUCENS PALSY | EXPANSION OF CAROTID CANAL HOMOGENEOUS ENHANCEMENT T2 HYPERINTENSE HETEROGENEOUS | CAROTID CANAL WITH CAVERNOUS SINUS FREE | ENCASING TO THE ICA | duv | PETROUS APEX |
| PRESENT CASE | INTERNAL CAROTID PLEXUS | 13 | MAN | HEARING LOSS HEADACHE VERTIGO FACIAL PALSY | EXPANSION OF CAROTID CANAL T1 ISOINTENSE WITH HOMOGENEOUS ENHANCEMENT T2 HYPOINTENSE HETEROGENEOUS WHITOUT RESTRICTED DIFFUSION | CAROTID CANAL WITH CAVERNOUS SINUS FREE | SUPERO-LATERAL TO THE ICA / ICA DISPLACED INFERO-MEDIALLY | 4 | CAROTID CANAL |
| 68 | MAXIMO | ||||||||
| 13 | MÍNIMO |
Conclusion
Schwannoma of the lateral aspect of the internal carotid plexus is an unusual tumor, nevertheless, it must not be forgotten by otolaryngologists, radiologists and neurosurgeons. Reviewing previous cases, we conclude that this entity occurs in men and women with ages ranged from 13 to 35 years old, and that, there is no difference in imaging studies between temporal schwannomas and those found elsewhere.
We also saw that everyone was treated with surgery, only one had favorable results, although radiosurgery, radiotherapy or combination of these may also be used in treatment. So, our case describes the fourth petrous schwannoma originated in the lateral aspect of the internal carotid plexus, the youngest patient reported with this condition and the only one to appear with peripheral facial paralysis.
Declarations
Funding: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship.
References
- Skolnik AD, Loevner LA, Sampathu DM, et al. Cranial nerve schwannomas: Diagnostic imaging approach. Radiographics. 2016; 36; 1463-1477.
- Ture U, Seker A, Kurtkaya O, Pamir MN. Internal carotid plexus schwannoma of the cavernous sinus: Case report. Neurosurgery. 2003; 52: 435-439.
- Hamilton JD, Demonte F, Ginserg LE. Imaging of carotid canal sympathetic plexus schwannoma. American Journal of Neuroradiology. 2011; 32: 1212-1215.
- Tamura R, Takahashi S, Kohno M, Kameyama K, Fujiwara H, et al. Intraosseous Schwannoma of the Petrous Apex. Journal of neurological surgery reports. 2015; 76:135-139.
- Takase H, Araki K, Seki S, Takase K, Murata H, Kawahara N, et al. Unique Diagnostic Features and Surgical Strategy for Intracranial Carotid Sympathetic Plexus Schwannoma: Case Report and Literature Review. World neurosurgery. 2017; 98: 876 (e1-876.e8)
- Goiney C, Bhatia R, Auerbach K, Norenberg M, Morcos J. Intraosseous schwannoma of the petrous apex. Journal of radiology case reports. 2011; 5: 8-16.
- Solodnik P, Som PM, Shugar JM, McDaniel SL. Intraosseous petrous apex neuroma: CT findings. Journal of computer assisted tomography. 1986; 10: 1027-1029.
- Horn KL, Hankinson HL, Nissen AJ, et al. Primary schwannoma of the petrous apex. Skull base surgery. 1995; 5: 261-268.
- Goudihalli SR, Goto T, Bohoun C, et al. Sympathetic Plexus Schwannoma of Carotid Canal: 2 Cases with Surgical Technique and Review of Literature. World neurosurgery. 2018; 118: 63-68.