
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Disseminated histoplasmosis: A threatening
emergent disease in Tunisia
Z Guesmi2,1*; B Mahdi2,1; A Kallel3,1; I Chelly4,1; T Badri5,1 ; S Haouet4,1; K Kallel3,1; A Berriche2,1; L Ammari2,1;
R Abdelmalek2,1; B Kilani2,1
1University of Tunis El Manar, Faculty of Medicine of Tunis, Tunisia.
2Infectious Diseases Department, la Rabta Hospital, Tunis, Tunisia.
3Parasitology-Mycology Laboratory, la Rabta Hospital, Tunis, Tunisia.
4Anatomo-Pathology Laboratory, la Rabta Hospital, Tunis, Tunisia.
5Dermatology Department, Habib Thameur hospital, Tunis, Tunisia.
*Corresponding Author : Z Guesmi
Infectious Disease Department, la Rabta Hospital, Tunis, Tunisia.
University of Tunis El Manar, Faculty of Medicine of Tunis, Tunisia.
Email: zeinebguesmi92@gmail.com
Received : Mar 15, 2023
Accepted : Mar 29, 2023
Published : Apr 05, 2023
Archived : www.jcimcr.org
Copyright : © Z Guesmi (2023).
Abstract
Introduction: Histoplasmosis is an infection due to a dimorphic fungus Histoplasma capsulatum. In Tunisia, there is no cases described among native Tunisians, but it is emerging as an exotic imported infection from Sub-Saharan Africa.
Methods: We reported the case of an Ivorian woman living with HIV, hospitalized at infectious diseases department in 2020 for disseminated histoplasmosis.
Case: A 37-year-old Ivoirian woman, living in Tunisia for 7 months, infected with HIV, presented with an impairment in general state, weakness, anorexia, and weight loss, evolving for 10 days. She was febrile, cachectic, and dehydrated. She had an oral candidiasis and a general skin eruption. Laboratory findings showed a pancytopenia. CRP was at 40 mg/l, ferritin was at 2201 ng/ml, LDH at 450 U/l. Lymphocyte T CD4 count was deeply low at 1 cell/μl. A skin biopsy of a nodular lesion was realized, and histology exam concluded to histoplasmosis. The mycological examination of skin smear stained with May Grunwald Giemsa, showed small yeasts typical of Histoplasma capsulatumvarcapsulatum. She received amphotericin B 1 mg/kg/day. Outcome was initially satisfactory but on the 8th day of treatment, she presented a bleeding syndrome with impairment in hemodynamic, neurologic, and respiratory state. Despite reanimation, she dead.
Conclusion: The presentation of histoplasmosis is not specific, but it must be suspected in immunocompromised patients coming from endemic area.
Keywords: Disseminated histoplasmosis; HIV infection; Histoplasma capsulatum; Tunisia; Emergent infection; Immigrant.
Citation: Guesmi Z, Mahdi B, Kallel A, Chelly I, Badri T, et al. Disseminated histoplasmosis: A threatening emergent disease in Tunisia. J Clin Images Med Case Rep. 2023; 4(4): 2358.
Introduction
Histoplasmosis is an infection due to a dimorphic fungus Histoplasma capsulatum. It was firstly discovered in 1906 by Samuel T Darling [1]. It is a telluric fungus, mainly transmitted by inhaling microconidia, more rarely by digestive pathway or skin excoriation. Some exceptional cases of transmission after liver or kidney transplantation have been reported [2,3].
It is endemic in parts of USA (Ohio and Mississippi valleys), Mexico, Central and South America, South-East Asia, India, China, Australia, parts of Europe (especially Italy) and Sub-Saharan-Africa [4]. In 2017, the annual incidence of disseminated histoplasmosis worldwide was 100,000 cases [5].
There are two varieties of Histoplasma capsulatum: Histoplasma capsulatum var capsulatum, the most common and Histoplasma capsulatum var duboisii or Histoplasma africana which is isolated only in Africa.
For immunocompetent patients, it is mainly responsible of asymptomatic forms or non-specific signs. However, in case of immunosuppression with HIV, immunosuppressive drugs, or aged patients, it may cause a severe infection that compromises vital prognosis and requires an urgent treatment.
In Tunisia, there is no cases described among native Tunisians, but it is emerging as an exotic imported infection from Sub-Saharan Africa.
The aim of our paper is to describe the clinical, para-clinical and outcomes of this infection by reporting a case of Ivorian woman living with HIV, hospitalized at infectious diseases department in 2020.
Clinical case
We report the case of a 37-year-old Ivoirian woman, who had been living in Tunisia for 7 months. HIV infection was recently discovered after a rapid test screening. She presented to our department with an impairment in general state, weakness, anorexia, and weight loss, evolving for 10 days. She was also complaining from generalized skin eruption, cough and vomiting without diarrhea.
Physical examination revealed a febrile, cachectic, and dehydratedpatient. She had an oral candidiasis and many maculopapular, pustularskin lesions and nodules on the face, purpuric lesions on the shoulders, and hyperpigmented macules on the back, trunk, and upper extremities (Figures 1A,B).
Her respiratory rate was by 22 cycles/min. Pulmonary auscultation was normal. She hada tachycardia at 110 pulse/mn, arterial pression was 90/60 mmHg.
The abdomen was tender. Liver length was at 18 cm. She had a splenomegaly.
Laboratory findings showed an anemia at 4.2 g/dL, leucopenia at 1130/ mm3, lymphopenia at 120/ mm3, neutropenia at 940/ mm3 and thrombopenia at 76,000/ mm3. CRP was at 40 mg/L, ferritin at 2201 ng/mL and LDH at 450 U/L. The other parameters were normal. Lymphocyte T CD4 count was deeply low at 1 cell/μL. The hepatitis B and C, leishmaniasis, toxoplasmosis and syphilis serologies were negative. Chest radiography was normal.
The body CT scan showed cervical cellulitis and fasciitis, bilateral non-necrotic cervical and axillary lymph nodes, a calcified left latero-basal micronodule with some centro-lobular emphysema bubble and hepato-splenomegaly.
She was rehydrated and had received a transfusion, so her state was stabilized.
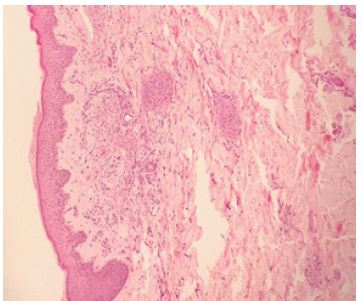
A skin biopsy of a nodular lesion was realized, and histology exam showed the presence of necrotic collagen lesions with numerous rounded, basophilic microorganisms. These microorganisms were intra- and extracellular taking Grocott and PAS, compatible with histoplasmosis (Figure 2).
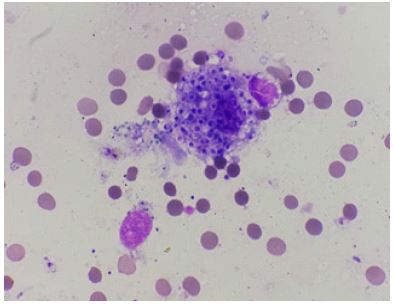
The mycological examination of skin smear stained with May Grunwald Giemsa, showed small yeasts typical of Histoplasma capsulatumvarcapsulatum (Figure 3). It was a disseminated histoplasmosis, so she was treated with amphotericin B 1 mg/kg/day. In addition, digestive endoscopy showed an extended esophagus candidiasis. No other treatment was associated. Outcome was initially satisfactory but on the 8th day of amphotericine B, she presented a bleeding syndrome with impairment in hemodynamic, neurologic, and respiratory state. Despite reanimation, she dead.


Discussion
To our knowledge, we have reported the second case of disseminated histoplasmosis in Tunisia. It’s an imported infection in our country but it’s endemic in other countries such as sub-Saharan Africa, the origin of our patient. The mean age of patients infected in literature is by 35.4 years (18-70) [6]. The male gender was mainly touched [6].
After inhalation of microconidia, they reach alveoli where they transform into yeast. These yeasts are phagocytized by the alveolar macrophage where they multiply. For immunocompetent host, macrophages can destroy the fungal particles in 10 to 14 days by forming necrosis at the infected sites, then caseum and fibrosis. However, for immunocompromised host, the infection can progress and may reach all organs. So, clinical presentation is polymorph and not specific.
Impairment in general state with fever were the main general symptoms in our case. In literature, these symptoms were reported in 83% of cases [7].
Our patient had an extensive generalized skin eruption. This symptom was reported only in 6% in literature. Our first case had no skin involvement [8]. Lesions were various and not specific with papular, macular, nodular, and ulcerative lesion. A Brazilian study had collected 36 patients living with HIV who presented histoplasmosis with skin eruption [9]. It was generalized in 58.3% of cases. Anisolated face localization was found in 27.8% of cases. An only upper and lower limb localization was reported in 8% of cases. Two patients had a trunk localization. A tumor syndrome was also reported: splenomegaly in 12 to 19% [10], hepatomegaly was revealed in 26 to 32% [6] and adenopathy in 35% to 48% of cases [7,11]. Other presentations were also described: Respiratory symptoms such as cough, thoracic pain, dyspnea revealed in 47% of cases in the study of Nacher and al [11], and neurological signs such as meningitis, encephalitis revealed in 20% of cases.
Laboratory findings were also nonspecific. A perturbation in CBC was mainly revealed due to infiltration of the bone marrow by histoplasma fungus or in contest of histiocyticsyndrome that may complicate the infection [13-16]. Kidney failure was also reported. A study showed that an impaired kidney function with creatinine above 21 mg/l is predictive of a severe form of infection [17]. LDH level above twice time normal, had a prognostic value and is associated with high mortality rate. Ferritin value > 10000, is specific of histoplasmosis and indicate to starturgent treatment without mycologic or histologic proof [18].
The gold standard diagnosis is to isolate histoplasma capsulatum in culture or direct exam with a sensitivity of 89.5% or in anatomopathological exam with a sensitivity of 78.3% [19]. Specific staining was used in mycologic exam especially MGG, GMS and PAS [20]. Culture shows especially the dimorphic character of the fungus by demonstrating transformation from yeast form to mycelian one [20]. But it required a special laboratory with a high biosecurity which is not available in our hospital.
Detection of antigen in plasma and/or urine or any other biologic liquidis a sensitive method which can be used for the diagnosis of histoplasmosis. The sensitivity of the test in urine is up to 100% and 94.2% in plasma but this method is only available in referral lab in Indianapolis [21].
Serology is another diagnosis method with a sensitivity of 88.5% [21], but antibodies can be isolated far from acute infection. PCR can be used for diagnosis; it offers a good specificity and sensitivity of 98.7% and 95.4% respectively [22].
Histoplasmosis occurs at an advanced state of HIV infection. Patients with disseminated histoplasmosis have a lymphocyte T CD4 count< 150 cells/μl [13]. Like in our case histoplasmosis can be associated with other opportunistic infection: tuberculosis in 70% of cases [23], toxoplasmosis 13% [11], pneumocystosis 13% [24], cytomegalovirus disease 9% [25]. For that, an exhaustive investigation is required in these cases.
Amphotericin B deoxycholate is the referral treatment for histoplasmosis with 0.7 to 1 mg/kg/day. Liposomal form can be used when available with 3 mg/kg/day [26]. Studies demonstrate that liposomal form is associated with better prognosis [54]. It must be retained at least for two weeks until improvement of general state and possibility of oral use.
For the switch, Itraconazole is the best option. It should be taken 200 mg three times per day for reaching steady state rapidly than 200 mg twice a day. Itraconazole have multiple interactions with antiretroviral therapy like efavirenz and lopinavir/ritonavir that must be checked to choose the better dosage and avoid altered efficiency and organ impairments.
Treatment should be retained for at least 12 months. It can be stopped after accomplishing some conditions; regular administration of treatment, LT CD4 > 150 cells/μl, HIV viral load < 400 copies/ml and urine antigen < 2 ng/ml.
A long-term treatment is indicated with itraconazole 200 mg/day if immunosuppression is persistent or in case of recurrent histoplasmosis despite a well-managed treatment [25].
Disseminated histoplasmosis in patient living with HIV is a serious infection. It is associated with a mortality estimated at 39% within three months of diagnosis [14]. This mortality is due to several factors, including the immunosuppressive condition, delayed diagnosis, co-infection with other opportunistic diseases, and critical complications, especially histiocytic syndrome, which can complicate 45% of cases of disseminated histoplasmosis [29].
Conclusion
Histoplasmosis was unknown in Tunisia until 2017 [8]. However, the increasing number of sub-Saharan African immigrants leads to think about it in any immunocompromised patient, in particular a patient living with HIV, having a low lymphocyte T CD4 count and complaining from cutaneous profuse nodules, lymph nodes, pancytopenia, or histiocytic syndrome. It is probably an underestimated pathology in our country.
The non-specific clinical presentation that can mimic several other pathologies like tuberculosis can be responsible for a delay in diagnosis and treatment which can worsen the prognosis and increase mortality.
References
- Darling ST. A protozoon general infection producing pseudotubercles in the lungs and focal necrosis in the liver, spleen, and lymph nodes. Am Med Assoc. 1906; 46: 1283-1285.
- Botterel F, Romand F, Saliba F. A case of disseminated histoplasmosis likely due to infection from a liver allograft. Eur J Clin Microbiol Infect Dis. 1999; 18: 662-664.
- Limaye AP, Connelly PA, Sagar M. Transmission of histoplasma capsulatum by organ transplantation. N Engl J Med. 2000; 343: 1163-1166.
- Wheat LJ, Azar MM, Bahr NC. Histoplasmosis. Infect Dis Clin North Am. 2016; 30: 207-227.
- Bongomin F, Gago S, Oladele RO, Denning DW. Global and multi-national prevalence of fungal diseases-estimate precision. J Fungi. 2017; 3: 57.
- Cano Torres JO, Olmedo Reneaum A, Esquivel Sánchez JM, Camiro Zuñiga A, Pérez Carrisoza A. Progressive disseminated histoplasmosis in Latin America and the caribbean in people receiving highly active antiretroviral therapy for HIV infection: A systematic review. Med Mycol. 2019; 57: 791-799.
- Nacher M, Valdes A, Adenis A, Blaizot R, Abboud P, Demar M, et al. Disseminated histoplasmosis in HIV-infected patients: A description of 34 years of clinical and therapeutic practice. J Fungi. 2020; 6: 164.
- N Fakhfakh, R Abdelmalek, S Aissa, A Kallel, Y Boudawara, et al. Disseminated histoplasmosis diagnosed in the bone marrow of an HIV-infected patient: First case imported in Tunisia. J Mycol Med. 2018; 28: 211-214.
- Cunha VS, Zampese MS, Aquino VR, Cestari TF, Goldani LZ, et al. Mucocutaneous manifestations of disseminated histoplasmosis inpatients with acquired immunodeficiency syndrome: Particular aspects in a Latin-American population. Clin Exp Dermatol. 2007; 32: 250-255.
- Huber F, Nacher M, Aznar C. AIDS-related histoplasma capsulatum var. capsulatum infection: 25 years’ experience of French Guiana. AIDS. 2008; 22: 1047-1053.
- Chiaruzzi M, Adenis A, Bonifay T, Djossou F, Bretagne S, Lanternier F, et al. Épidémiologie des infections à Histoplasmacapsulatumsp diagnostiquées en France métropolitaine. Étude transversale multicentrique 2007-2018. Med Mal Infect. 2020; 50: 5.
- Therby A, Lefort A, Dupont B, Lortholary O. Actualités sur l’histoplasmose à histoplasmacapsulatum variété capsulatum [En ligne]. La Lettre de l’infectiologue [citedin 13/12/2020] ; [environ 7 écrans]. Disponible : https://www.edimark.fr/Front/frontpost/getfiles/9052.pdf
- Myint T, Leedy N, Villacorta Cari E, Wheat LJ. HIV-Associated histoplasmosis: Current perspectives. HIV AIDS. 2020; 12: 113-125.
- Baddley JW, Sankara IR, Rodriquez JM, Pappas PG, Many WJ, et al. Histoplasmosis in HIV-infected patients in a southern regional medical center: poor prognosis in the era of highly active antiretroviral therapy. Diagn Microbiol Infect Dis. 2008; 62: 151–156.
- Rao R. Recurrent primary cutaneous histoplasmosis in a post-renal transplant patient. J Nephrol Ren Transplant. 2008; 1: 53–58.
- Kauffman CA. Histoplasmosis: A clinical and laboratory update. ClinMicrobiol Rev. 2007; 20: 115–132.
- Wheat LJ, Chetchotisakd P, Williams B, Connolly P, Shutt K, Hajjeh R, et al. Factors associated with severe manifestations of histoplasmosis in AIDS. Clin Infect Dis. 2000; 30: 877–881.
- Kirn DH, Fredericks D, McCutchan JA, Stiles D, et al. Serum ferritin levels correlate with disease activity in patients with AIDS and disseminated histoplasmosis. Clin Infect Dis.1995; 21: 1048–1049.
- Mukhopadhyay S, Katzenstein AL. Biopsy findings in acute pulmonary histoplasmosis: unusual histologic features in 4 cases mimicking lymphomatoid granulomatosis. Am J SurgPathol. 2010;34(4):541-6.
- Zanotti P, Chirico C, Gulletta M, Ardighieri L, Casari S. Disseminated histoplasmosis as AIDS-presentation. Case report and comprehensive review of current literature. Mediterr J Hematol Infect Dis. 2018; 10: e2018040.
- Myint T, Anderson AM, Sanchez A. Histoplasmosis in patients with human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS): Multicenter study of outcomes and factors associated with relapse. Medicine. 2014; 93: 11–18.
- Kok J, Chen SC, Anderson L. Protein-losing enteropathy and hypogammaglobulinaemia as first manifestations of disseminated histoplasmosis coincident with nocardia infection. J Med Microbiol. 2010; 59: 610-613.
- Agudelo CA, Restrepo CA, Molina DA. Tuberculosis and histoplasmosis co-infection in AIDS patients. Am J Trop Med Hyg. 2012; 87: 1094–1098.
- Carreto Binaghi LE, Morales Villarreal FR, Garcia De La Torre G, et al. Histoplasma capsulatum and Pneumocystis jirovecii coinfection in hospitalized HIV and non-HIV patients from a tertiary care hospital in Mexico. Int J Infect Dis. 2019; 86: 65–72.
- Caceres DH, Tobon AM, Restrepo A, Chiller T, Gomez BL, et al. The important role of co-infections in patients with AIDS and progressive disseminated histoplasmosis (PDH): A cohort from Colombia. Med Mycol Case Rep. 2018; 19: 41–44.
- Wheat LJ, Freifeld AG, Kleiman MB. Clinical practice guidelines for the management of patients with histoplasmosis: 2007 update by the infectious diseases society of America. Clin Infect Dis. 2007; 45: 807–825.
- Johnson PC, Wheat LJ, Cloud GA. Safety and efficacy of liposomal amphotericin B compared with conventional amphotéricine B for induction therapy of histoplasmosis in patients with AIDS. Ann Intern Med. 2002; 137: 105–109.
- Weat J, Hafner R, Korzun AH, et al. Itraconazole treatment of disseminated histoplasmosis in patients with the acquired immunodeficiency syndrome. AIDS clinical trial group. Am J Med. 1995; 98: 336–342.