
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Causality or coincidental: The first case report of acute
inflammatory demyelinating polyneuropathy following
COVID-19 vaccination in the Philippines
*Corresponding Author : Jon Stewart Dy
Department of Medicine, Quezon City, Philippines
Email: jonjondy@gmail.com
Received : Mar 13, 2023
Accepted : Mar 30, 2023
Published : Apr 06, 2023
Archived : www.jcimcr.org
Copyright : © Stewart Dy J (2023).
Abstract
Since the start of the COVID-19 pandemic in December 2019, worldwide COVID-19 vaccination campaigns have been done to prevent the further spread of COVID-19. While COVID-19 infection has been found to have multiple neurological complications, an increased risk of Guillain-Barre’ Syndrome (GBS) has been attributed to COVID-19 vaccination. Here we report the first case of COVID-19 vaccine-related GBS in the Philippines.
Citation: Stewart Dy J. Causality or coincidental: The first case report of acute inflammatory demyelinating. J Clin Images Med Case Rep. 2023; 4(4): 2359.
Introduction
Guillain-Barre’ Syndrome (GBS) is the most common cause of acute or subacute generalized paralysis in clinical practice, affecting children and adults of all ages, with a slight male predominance. In almost two thirds of cases, mild respiratory or gastrointestinal infection precede neuropathic symptoms by one to three weeks [1]. While most cases of GBS are preceded by infection, a modest risk of GBS has been attributed to vaccinations such as the yearly influenza vaccine and meningococcal vaccine [1,2]. This raises concern that the current worldwide COVID-19 vaccination campaign can lead to increased incidence of GBS. Indeed, there have been case reports of GBS attributed to COVID-19 vaccines (Johnson and Johnson, Pfizer, AstraZeneca) that have been published in United States, United Kingdom, Israel, Egypt, Austria and Qatar. Based on these published case reports, the onset from the time of vaccination to the development of neuropathic symptoms can be as short as one day to as much as twenty-one days [3-9,1]. To date, there have been no published case reports in the Philippines regarding COVID-19 vaccine and the development of neuropathic symptoms attributed to AIDP. Here we report the first case of AIDP in the Philippines after receiving the first dose of AstraZeneca COVID-19 vaccine.
Case report
A 45-year old female with good baseline functional capacity who was independent on all her activities of daily living, with a history of essential hypertension was given her first dose of AstraZeneca vaccine on May 24, 2021. She remained well without any respiratory or gastrointestinal symptoms until 10 days after vaccination when she started experiencing severe holocranial band-like headache, which eventually resolved with bedrest and as needed pain reliever. The next day (11 days after vaccination), she then noted paresthesia over both hands and feet with weakness of the proximal bilateral upper and lower Extremities. She would have difficulty raising her arms above her head and ascending up the stairs. By the next day, there would be persistence of Weakness of the proximal bilateral upper and lower Extremities, where she would eventually seek Emergency care consults at two local hospitals Where work-ups (complete blood count, Electrolytes, cardiac enzyme, thyroid function tests, Renal and liver function tests, plain whole Abdominal CT scan, cranial CT scan with contrast) Were unremarkable and she was managed as a Case of hypertensive urgency. Her blood pressure Ranges during this time was 160-180/100. She was the discharged with dual antihypertensive medications (Amlodipine and Losartan) without improvement of symptoms. Interim, there would be worsening of symptoms for which she now required assis-tance when ambulating, now with generalized body aches, bilateral ptosis, slurring of speech and dysphagia (both solids and liquids). Her physical examination on presentation revealed normal mental status while cranial nerve examination showed bilateral ptosis (left more than the right eye), bilateral lateral rectus palsy (left more than the right), decreased sensation (light touch, pinprick, temperature) over the distribution of the trigeminal nerve, facial diplegia, weak palatal elevation and dysphonia. Motor examination shows muscle weakness of 3/5 on the proximal bilateral upper and lower limbs, and 4/5 in the distal bilateral upper and lower limbs. Sensory examination shows decreased sensation (light 2 touch, pinprick, temperature, vibration) involving the dorsal and palmar aspect of both hands (until the wrist area), and the dorsal and plantar aspect of both feet (until the ankle area). No dysmetria nor dysdiachokinesia was noted. Reflex testing shows hyporeflexia in the bilateral upper extremities and areflexia in the bilateral lower extremities. Routine labs showed euvolemic hyponatremia sec-ondary to syndrome of inappropriate ADH secretion. RTPCR for SARS-CoV2 was negative on admission. Lumbar puncture was not performed due to patient refusal. Cranial MRI with contrast was normal while whole spinal MRI with contrast showed unremarkable results. She was admitted to the progressive care unit and elec-trophysiologic studies done one day after admission showed absent bilateral sensory median response while median and ulnar motor studies showed slowed conduction velocity and prolonged distal motor latency, con-duction block in the bilateral ulnar and left peroneal nerve, diffuse low amplitude responses, absent F responses, increased insertional activity in the left deltoid with all muscles showing reduced recruitment. These findings are compatible with the electrophysiologic criteria of Acute Inflammatory Demyelinating Polyneuropathy (AIDP). She was then treated with intravenous Immunoglobulin (2 g/kg over 5 days) starting on June 12, 2021 (18 days after vaccination, eight days after onset of neuropathic symptoms). The patient did not show any signs of respiratory compromise and clinical improvement was seen after the patient completed five days of IVIG. No complications were noted during and after the treatment. The patient received daily physical, occupational and speech therapy during the hospital stay with improvement in motor strength and she was discharged to rehabilitation 14 days after admission. She was referred to outpatient Neurology Clinic for follow-up electrophysiologic studies to be done in four weeks.
Discussion
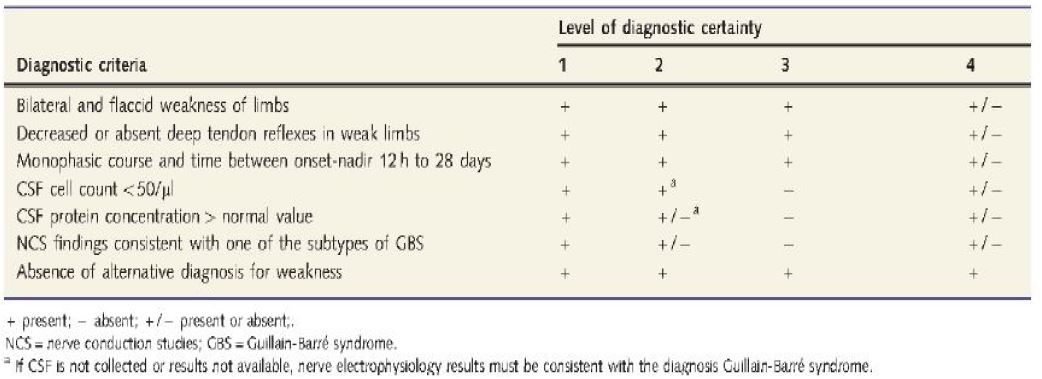
Guillain-Barre Syndrome (GBS) is associated with numerous bacterial and viral infections [1]. The pathogenesis involves the production of an immune response secondary to antecedent infection or vaccination, which in turn cross-reacts with peripheral nerve components because of sharing of cross-reactive epitopes (molecular mimicry). Immune response can be directed against the myelin or the axon, the latter of which cause the axonal vari-ants of GBS which are associated with a worse prognosis and slower recovery time [2]. The Brighton criteria is a diagnostic tool that can in the diagnosis of GBS (Figure 1) [11]. The most important diagnostic aids in GBS include Cerebrospinal Fluid (CSF) analysis and electrophysiologic studies. CSF analysis will show normal pressure, acellular or few lymphocytes and increased CSF protein secondary to widespread inflammatory disease of the nerve roots. This is compatible with albumincy to logic dissociation seen in GBS. Electrophysiologic criteria of GBS include prolonged distal motor latency, slowed conduction velocity, absent F responses and conduction block. At least three of the four electro physiologic criteria are needed for the diagnosis of GBS [1,2,11]. Spinal MRI with gadolinium contrast will show enhancement of the nerve roots of the cauda equine [2]. Since the start of the global COVID-19 pandemic in December 2019, global mass vaccination campaigns have been done to mitigate the spread of COVID-19 infection. The FDA-approved COVID- 19 vaccines are either inactivated or live messenger RNA vaccines that enter the human cell to allow identification of the spike protein found on the surface of SARS-CoV2 virus [3]. The human body then produces antibodies that recognize and kill the virus. In a small subset of patients, this immune response leads to the production of antibodies against myelin and axon, thereby causing GBS. The proposed pathophysiology of vaccine associated GBS is an immune-mediated. Hy-persensitivity to the solvent (polyethylene glycol) [5]. GBS may be seen in patients within six weeks after receiv-ing a first dose of 10 weeks after a second dose [3]. Because of the limited case reports, no guidelines on the optimal treatment of vaccine-associated GBS are available. Most cases have been treated with IVIG (2 g/kg over 3-5 days) [3,5-10].
Conclusion
In summary, we report the first case of COVID-19 post vaccine associated GBS in the Philippines. Rare occurrences of COVID-19 vaccine-related neuromuscular complications are possible. Any serious adverse reaction must be reported to facilitate continuous safety evaluation and to minimize vaccine hesitancy. It is important to emphasize to patients and to the public that temporal association does not always imply causality. Further studies are needed to better elaborate the neurological complications after COVID-19 vaccination and whether a causal relationship between vaccination and neurological complications can be established. With the ongoing pandemic and worldwide mass vaccination campaigns, it is important for clinicians to recognize the other adverse effects associated with COVID-19 vaccination. Lastly, it is important to highlight that the benefits of COVID-19 vaccination outweigh the risks and possible adverse effects associated with vaccination in order to limit and mitigate the further spread of COVID-19 infection.
Declarations
Acknowledgements: We would like to thank Teodoro Cruz, MD and Lina Laxamana, MD for manuscript formatting and proof reading of the article. We would also like to express gratitude to the comments and assistance with the electrophysiological studies by Ludwig Damian, MD.
Disclosures: Human subjects: Consent was obtained by all participants in this study.
Conflicts of interest: None of the authors have any conflicts of interest to disclose.
Payment/services
Information: All authors have declared that no financial support was received from any organization for the submitted work.
Data availability statement: Data sharing is not applicable to this article as no datasets were generated or analyzed during the current study.
References
- Ropper AH, Adams R, Victor M, & Samuels MA. Adams and Victor’s principles of neurology. Mc Graw Hill Medical. 2019; 1309-1328.
- Up To Date. GBS: Epidemiology, Pathogenesis, Clinical Features and Diagnosis, Prognosis.
- Loza, AMM, Holroyd KB, Johnson SA, Pilgrim DM, Amato AA. Guillain-Barré syndrome in the place bo and active arms of a COVID-19 vaccine clinical trial: Temporal 4 associations do not imply causality. Neurology. 2021; 96: 1052-1054.
- Waheed S, Bayas A, Hindi F, Rizvi Z, Espinos PS. Neurological complications. 2021. of COVID-19: Guillain-Barre syndrome following Pfizer COVID-19 vaccine. Cureus. 2021; 13.
- Waheed W, Carey ME, Tandan S R, Tandan R. Post COVID-19 vaccine small fiber neuropathy. Mus-cle & Nerve. 2021; 64: E1.
- Patel SU, Khurram R, Lakhani A, Quirk B. Guillain-Barre syndrome following the first dose of the chimpanzee adenovirus-vectored COVID-19 vaccine, ChAdOx1. BMJ Case Reports CP. 2021; 14: e242956.
- Ogbebor O, Seth H, Min Z, Bhanot N, et al. Guillain-Barré syndrome following the first dose of SARS-CoV-2 vaccine: A temporal occurrence, not a causal association. ID Cases. 2021; 24: e01143.
- Razok A, Shams A, Almeer A, Zahid M. Post-COVID-19 vaccine Guillain-Barré syndrome; First report-ed case from Qatar. Authorea Preprints. 2021.
- Finsterer J. Exacerbating Guillain–Barré Syndrome Eight Days after Vector-Based COVID- 19 Vac-cination. Case Reports in Infectious Diseases. 2021.
- Azam S, Khalil A, Taha, A. Guillain-Barré Syndrome in a 67-year-old Male Post COVID-19 Vaccina-tion (Astra Zeneca). American Journal of Medical Case Reports. 2021; 9: 424-427.
- Ghazanfar, et al. Significance of Brighton Criteriia in the Early Diagnosis and Management of GBS. Cureus. 2020; 12.
- Center for Disease Control and Prevention. Vaccine Safety. Retrieved from https://www.cdc.gov/vaccinesafety/ensuringsafety/ monitoring/vaers/index.html. Accessed 2021.