
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
Recurrent pneumococcal meningitis due to
an acquired anatomical defect
Nikhila Aimalla, MD1*; Isaac Boyack, MD2
1Department of Medicine-Pediatrics, Marshfield Clinic Health System, Marshfield, WI, USA.
2Department of Neuroradiology, Marshfield Clinic Health System, Marshfield, WI, USA.
*Corresponding Author : Nikhila Aimalla
Department of Medicine-Pediatrics, Marshfield Clinic Health System, Marshfield, WI, USA.
Email: aimalla.nikhila@marshfieldclinic.org
Received : Mar 14, 2023
Accepted : Mar 30, 2023
Published : Apr 06, 2023
Archived : www.jcimcr.org
Copyright : © Aimalla N (2023).
Citation: Aimalla N, Boyack I, et al. Recurrent pneumococcal meningitis due to an acquired anatomical defect. J Clin Images Med Case Rep. 2023; 4(4): 2360.
Description
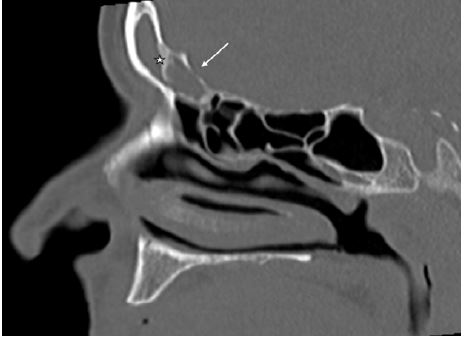
A 66-year-old woman with type 2 diabetes, chronic sinusitis, chronic smoking, and a history of pneumococcal meningitis in 2019 presented to the hospital in October 2022 after being poorly responsive at home. On arrival, she was somnolent with a GCS of 5. CT head revealed mucosal thickening of the left maxillary sinus. Blood cultures were obtained, and she was administered intravenous ceftriaxone, vancomycin, ampicillin, and dexamethasone. Subsequent CSF analysis showed total nucleated cells of 19652/ uL, red blood cells of 8875/ uL, glucose of 56 mg/dl, and total protein of 1057 mg/dl. Blood cultures grew Streptococcus pneumoniae susceptible to ceftriaxone; the CSF culture was negative. We narrowed the antibiotics to high-dose ceftriaxone. She was current with pneumococcal vaccination. An evaluation of her immune system, including targeted genetic testing, was negative. CT of the sinuses without contrast (Figure 1) demonstrates complete opacification of the left frontal sinus with marked thinning and osseous defect (white arrow) in the posterior wall of the frontal bone. Osseous changes are atypical of acute rhinosinusitis and consistent with complicated paranasal sinus disease. Osteogenesis (white star) within the left frontal sinus suggests a chronic inflammatory component.
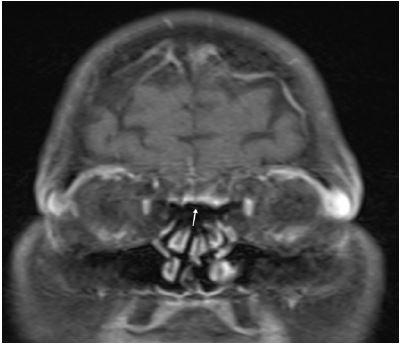
Coronal brain MRI (Figure 2) demonstrates abnormal meningeal thickening and enhancement (white arrow) along the floor of the anterior cranial fossa and cribriform plate just posterior to the frontal sinus defect seen on concurrent non-contrast CT of the sinuses. These findings are consistent with meningitis secondary to complicated acute bacterial rhinosinusitis. Recurrent bacterial meningitis is uncommon, occurring in 5% of meningitis cases [1]. It indicates the possibility of immunodeficiency or congenital or acquired anatomic defect [2]. She showed remarkable recovery after three weeks of antibiotic treatment. We started her on prophylactic cefpodoxime to prevent recurrent infection and referred her to a sinus center for surgical correction of the left frontal sinus osseous defect [3].
References
- Ter Horst L, Brouwer MC, van der Ende A, van de Beek D. Recurrent Community-Acquired Bacterial Meningitis in Adults. Clin Infect Dis. 2021;73: e2545-e2551.
- Sponsel C, Park JW. Recurrent pneumococcal meningitis. Postgrad Med. 1994; 95: 109-197.
- Anitua E, Alkhraisat MH, Miguel-Sánchez A, Orive G. Surgical correction of horizontal bone defect using the lateral maxillary wall: Outcomes of a retrospective study. J Oral Maxillofac Surg. 2014; 72: 683-693.