
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 4
Hypertensive encephalopathy in hereditary angioedema:
Concerns on bradykin in overflow
Solange OR Valle1; Sérgio D Dortas1; Guilherme Gomes AZIZI1; Rafael Esteves Carriço1; Maria Luiza Oliva Alonso1; Lara Brandão2
1Serviço de Imunologia, Hospital Universitário Clementino Fraga Filho (HUCFF-UFRJ), Rio de Janeiro, Rio de Janeiro, Brazil.
2Institutode Ressonância Magnética Lara Brandão, Rio de Janeiro, Brazil.
*Corresponding Author : Solange OR VALLE
Serviço de Imunologia, Hospital Universitário Clementino Fraga Filho (HUCFF-UFRJ), Rio de Janeiro, Rio de Janeiro, Brazil.
Email: solangervalle@gmail.com
ORCID ID: 0000-0001-5512-7349
Received : Mar 09, 2023
Accepted : Mar 31, 2023
Published : Apr 07, 2023
Archived : www.jcimcr.org
Copyright : © Valle SOR (2023).
Abstract
A 69-year-old woman with Hereditary Angioedema (HAE) due to deficient C1INH (Type I) was admitted to an orthopedic unit for a knee prosthesis infection. She subsequently developed angioedema in her eyelids, face, and hands, followed by a reduction in visual acuity that progressed to amaurosis within 48 hours. She then experienced a generalized tonic-clonic seizure and a reduction in consciousness, which required orotracheal intubation. Hypertensive Encephalopathy (HE) was suspected due to high blood pressure, and she was given Captopril as needed. Icatibant 30 mg was administered, and the ACE inhibitor was discontinued. The patient showed improvement in angioedema, neurological deficit, and cerebral edema on CCT.
Citation: Valle SOR, Dortas SD, Azizi GG, Carriço RE, Alonso MLO, et al. Hypertensive encephalopathy in hereditary angioedema: Concerns on bradykin in overflow. J Clin Images Med Case Rep. 2023; 4(4): 2361.
Introduction
Hereditary Angioedema (HAE) is a rare, potentially life-threatening disorder characterized by cutaneous and submucosal swelling. The most frequent type of HAE is HAE with deficiency of C1 Inhibitor (C1INH) due to mutations in the SERPING1 gene. Bradykinin is the main biological mediator of swelling, so glucocorticoids, antihistamines, and epinephrine are not effective [1,2]. Diagnosis can be challenging due to high clinical variability [1].
Case presentation
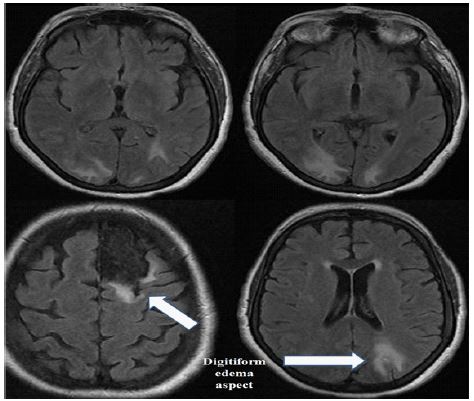
A 69-year-old woman with HAE due to deficient C1INH (Type I) was admitted to an orthopedic unit for a knee prosthesis infection. She subsequently developed angioedema in her eyelids, face, and hands, followed by a reduction in visual acuity that progressed to amaurosis within 48 hours. She then experienced a generalized tonic-clonic seizure and a reduction in consciousness, which required orotracheal intubation. Due to high blood pressure, Hypertensive Encephalopathy (HE) was suspected, and she was given Captopril as needed. Her diagnosis was confirmed at our outpatient clinic with low C4 and C1INH. HAE was also diagnosed in three of her cousins and her offspring. Icatibant and oxandrolone were prescribed for on-demand and prophylactic treatment, respectively. A CCT showed hypodense subcortical areas consistent with edema, mainly in the occipital lobes bilaterally and the left parietal lobe, along with partial sulci effacement, mainly in the high convexity and cerebellum. CT findings (Figure 1) were suggestive of HE.
Our ACARE (Angioedema Centers of Reference and Excellence) team was contacted, and the hypothesis of concomitant brain angioedema due to HAE was raised. Icatibant 30 mg was administered, and the ACE inhibitor was discontinued. The patient showed improvement in facial edema and was extubated after seven days without neurological deficit, and the amaurosis was resolved. A follow-up CCT showed complete resolution of cerebral edema.
Discussion
HE is an acute syndrome characterized by acute hypertension leading to various neurological symptoms and neuroimaging findings [3]. The neurological syndrome in HE is believed to be caused by vasogenic edema secondary to failure of cerebral autoregulation [4]. Protease-Activated Receptor 2 (PAR2) and Bradykinin subtype 2 receptor are up-regulated in HE, producing endothelium-dependent vasodilation [5].
HAE with C1INH deficiency is a condition characterized by recurrent angioedema linked with mutations in the SERPING1 gene leading to low levels of functional C1-INH in plasma. During acute swelling attacks, the kallikrein-kinin system is activated with the overproduction and accumulation of the vasoactive peptide bradykinin. Attacks may manifest spontaneously or be induced by various stimuli such as trauma, emotional stress, infections, menstruation, pregnancy, estrogen-based oral contraceptives, alcohol, extreme temperatures, use of ACE inhibitors, and gliptins [1,6]. The typical duration of such attacks is 3-5 days, and conventional treatments aimed at blocking histamine-mediated or mast cell-mediated angioedema such as glucocorticoids, antihistamines, and epinephrine are ineffective [1].
Conclusion
In conclusion, managing HAE patients and enabling them to lead a normal life requires the avoidance of severe attacks through early recognition, patient education, and family support. Health care professionals must be vigilant regarding potential triggers of HAE attacks. Fortunately, our patient responded well to icatibant (a bradykinin antagonist) and the removal of ACE inhibitors, indicating that edema persistence may be due to bradykinin accumulation. HAE patients should have access to written communication that can be shared with their healthcare providers, providing essential information about HAE, specific treatment options, monitoring, and emergency contact information for their HAE specialist. It is crucial to maintain constant vigilance to prevent and promptly treat preventable manifestations of HAE.
Declarations
Aknowledgement: This survey was carried out as part of the assistance provided by the Serviço de munologia, Hospital Universitário Clementino Fraga Filho (HUCFF-UFRJ)
Consent for publication: The authors allow this manuscript to be used freely for publication by this journal.
Competing interests: The authors declare that they have no conflicts of interest regarding this study
Funding sources: This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Statement of ethics: This research has been submitted and Approved by Comitê de Ética em Pesquisa do Hospital Universitário Clementino Fraga Filho (HUCFF-UFRJ), number CAAE 45067715.5.0000.5257.
References
- Busse PJ, Christiansen SC: Hereditary Angioedema. N Engl J Med. 2019; 382: 1136-1148.
- Paige D, Maina N, Anderson JT: Hereditary angioedema: Comprehensive management plans and patient support. Allergy Asthma Proc. 2021; 41: 38-42.
- Li Y, Gor D, Walicki D, Jenny D, Jones D, et al. Spectrum and potential pathogenesis of reversible posterior leukoencephalopathy syndrome. J Stroke Cerebrovasc Dis. 2012; 21: 873-882.
- Schwartz RB, Jones KM, Kalina P, Bajakian RL, Mantello MT, et al. Hypertensive encephalopathy: Findings on CT, MR imaging, and SPECT imaging in 14 cases. AJR Am J Roentgenol. 1992; 159: 379-383.
- Smeda JS, McGuire JJ, Daneshtalab N: Protease-activated receptor 2 and bradykinin- mediated vasodilation in the cerebral arteries of stroke-prone rats. Peptides. 2010; 31: 227-237.
- Steckelings UM, Artuc M, Wollschläger T, Wiehstutz S, Henz BM, et al. Angiotensin- converting enzyme inhibitors as inducers of adverse cutaneous reactions. Acta Derm Venereol. 2001; 81: 321-325.