
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 4
An unusual case of Entamoeba histolytica infection in a soldier
deployed in the Sinai Peninsula, Egypt
Aporosa Robaigau*; Ronald J Lovich; Edgie-Mark Co
Multinational Force and Observers, Sinai, Egypt.
*Corresponding Author : Aporosa Robaigau
Multinational Force and Observers, Sinai, Egypt.
Email: aporosa.robaigau@yahoo.com
Received : Mar 12, 2023
Accepted : Mar 31, 2023
Published : Apr 07, 2023
Archived : www.jcimcr.org
Copyright : © Robaigau A (2023).
Citation: Robaigau A, Lovich RJ, Co EM. An unusual case of entamoeba histolytica infection in a soldier deployed in the Sinai Peninsula, Egypt. J Clin Images Med Case Rep. 2023; 4(4): 2362.
Background
A 49-year-old male Fijian soldier with no significant past medical history presented with a one-week history of fever (39.5oC) and dyspnea with hypoxemia. A complete blood count showed leukocytosis (25,120/ mm3) with neutrophilia (84%), and chest imaging revealed interstitial pneumonia. SARS-CoV-2 tests showed positive RT-PCR test and mono-IgG serology and negative Rapid Antigen test. He was treated with amoxicillin, azithromycin, and acetaminophen for presumed community-acquired pneumonia.
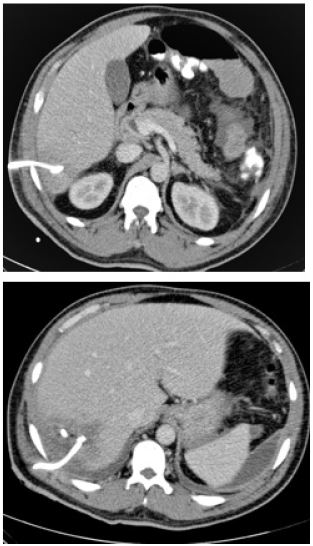
However, his fever continued over the following week, at which time he was evacuated to an Israeli hospital and was started on ceftriaxone and metronidazole. A CT scan performed at this time revealed multiple liver abscesses (Figures 1 and 2). Multiple drains were sited with an Interventional Radiology (IR) approach, which drained milky purulent discharge initially. Blood and abscess cultures were negative for bacterial growth, but Entamoeba histolytica was detected via PCR of abscess material. His fever resolved and abdominal pain improved, at which time ceftriaxone was discontinued. The drain discharge transitioned from a purulent to serosanguinous fluid, and the drains were removed on day 21. He was discharged with a prescription for an additional week of paromomycin and metronidazole Subsequent stool antigen and PCR tests were negative for E. histolytica, and the soldier returned to duty after a month of convalescence.

Discussion
This case describes E. histolytica liver abscesses in the setting of a COVID-19 infection. Globally, infections with E. histolytica protozoa are the third leading cause of death from parasites, although a large proportion of these infections are asymptomatic infections that can persist for months [1]. The parasite has a relatively simple life cycle, transitioning from trophozoite to cyst form, the latter being relatively resistant to chlorine and other cleaning agents. Clinical manifestations typically include diarrhea, dysentery, hepatic abscess formation, and, in extreme cases, fulminant colitis. Diagnostic modalities include examination for ova and parasites in the stool, serology, and RT-PCR, the latter considered the gold standard for diagnosis [2]. Treatment involves a 10-day course of the antiparasitics metronidazole, tinidazole, and nitazoxanide together with an intraluminal agent (e.g., paromomycin, iodoquinol, or diloxanide furoate). The pathogen can be challenging to diagnose and managein the austere settingsbecauseadvanced diagnostic modalities are not always available, and hygiene may be far from ideal.
In this case, the patient presented with clinical evidence of interstitial pneumonia and without gastrointestinal symptoms. There were no on-camp cases of E. histolytica infections six months prior to the patient’s arrival, although other cases had occurred in the past. The initial presentation with neutrophilia without overt eosinophilia was consistent with a bacterial infection, thus the initial management. In fact, eosinophilia is not a common feature of either symptomatic or asymptomatic E. histolytica [3]. So it is not a useful marker of infection. Other unusual features of this case include the multi-lobar nature of the liver abscess, necessitating multiple IR drains. Bacterial co-infections are common in E. histolytica abscesses given the invasive nature of the pathogen, although the continued resolution of symptoms after discontinuation of ceftriaxone for this patient suggests otherwise.
We suspect that the patient had an initial COVID-19 infection that masked the underlying E. histolytica infection that was potentially acquired prior to deployment to the Sinai. Although E. histolytica would have probably been diagnosed if the patient had presented with diarrheal symptoms given PCR availability at this location, this case highlights that the initial clinical presentation may not be obvious and thus requires advanced diagnostics not available in the austere setting. Even though the patient had a positive outcome, it is always important to consider parasitic diseases such as E. histolytica in undifferentiated fever in a deployed setting, especially in the COVID-19 era.
Disclaimers
The views expressed are those of the authors and do not necessarily reflect the official policy or position of Multinational Force and Observers, the U.S. Department of the Army, U.S. Department of Defense, or the U.S. Government.
References
- Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012; 380: 2095-2128.
- Roy S, Kabir M, Mondal D, et al. Real-time-PCR assay for diagnosis of Entamoeba histolytica infection. J Clin Microbiol. 2005; 43: 2168-2172.
- Yanagawa Y, Nagata N, Yagita K, et al. Clinical Features and Gut Microbiome of Asymptomatic Entamoeba histolytica Infection. Clin Infect Dis. 2021; 73: e3163-e71.