
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Eumycetoma: An unexpected diagnosis in Central Europe
Daniel Gödde1,3; Holger Schubert2; Stephan Störkel1,3
1Department of Pathology and Molecular Pathology, Helios University Hospital Wuppertal, 42283 Wuppertal, Germany.
2Centre for Orthopaedics and Rheumatology, Sankt Josef Hospital, 42105 Wuppertal, Germany.
3Department of Medicine, Faculty of Health, Witten/Herdecke University, 58448 Witten, Germany.
*Corresponding Author : Daniel Godde
Helios University Hospital Wuppertal, Department of Pathology and Molecular Pathology, Heusnerstr. 40, 42283 Wuppertal, Germany.
Tel: 0049-202-896 2850, Fax: 0049-202-896 2739;
Email: daniel.goedde@helios-gesundheit.de
Received : Feb 01, 2023
Accepted : Apr 03, 2023
Published : Apr 10, 2023
Archived : www.jcimcr.org
Copyright : © Gödde D (2023).
Abstract
Mycetomas are slow growing pseudotumors, which develop after trauma with an infection caused by bacteria or fungi. This localized infection in the cutis and subcutis is identified as eumycetoma or “Madura foot” when caused by fungi. Without proper treatment, bulky and obstructive tumors develop. These tumors form fistulas from which pus oozes, sometimes granular. Eumycetomas may also lead to bone destruction, but usually do not show dissemination. In temperate zones, the diagnosis of eumycetoma is rare.
A female Korean patient, 62 years old, presented to the orthopedic department with a subcutaneous, slow-growing tumor on her ankle. After surgical removal of the tumor, an eumycetoma caused by Fusarium solani was diagnosed by histopathological and molecular methods. Two years after the diagnosis, no complications have occurred. Correct identification of the pathogen is essential for treatment. In addition to a culture of the pathogen, a molecular approach is possible. While patients with bacterial infections and actinomycotic mycetomas require systemic antibiotic treatment, the treatment of eumycetomas depends on the extent of the infection and the pathogen. In this case, systemic antifugal treatment, with or without additional surgery, is advisable.
Keywords: Deep Mycosis; Eumycetoma; Madura foot; Fusarium solanionance.
Citation: Godde D, Schubert H, Störkel S. Eumycetoma: An unexpected diagnosis in Central Europe. J Clin Images Med Case Rep. 2023; 4(4): 2364.
Introduction
Mycetomas of the leg, also known as “Madura`s foot”, is typically seen as slowly growing, painless inflammatory pseudotumors. They develop after trauma, with the infection of bacteria (actinomycetomas) or fungi (eumycetomas), and occur most often in adults between the ages of twenty and forty. In 60-80% of cases, they occur on the leg, but can also affect any other part of the body. Geographically, the disease is most common in areas between latitudes 30 degree north and 15 degree south in tropical or subtropical climate. Risk factors include walking barefoot and agricultural work [1-6].
In moderate climates, such as in Germany, these lesions are extremely rare. However, the disease should be considered in patients from tropical areas that exhibit slow growing subcutaneous masses with fistulas, or in patients who exhibit the same after visiting tropical areas, especially if there has been an injury. Due to the slow progression of the lesion, there can be years, even decades between infection of the bacteria and diagnosis [1-3]. Initially, clinical findings are non-specific and there is no systemic reaction. In progressive mycetomas, the lesions can ulcerate and necrotize, and fistulas can develop with secretion of pus and granules, important clues for diagnosis. Even though mycetomas can lead to a destruction of adjacent bone, hematogenous dissemination usually does not occur [1,2].
Case presentation
A 62-year-old nurse of Korean descent living in Germany presented with a subcutaneous painless nodule, which had been present for about six months. The lesion was located between the lateral malleolus and the Achilles tendon of her left leg. The patient felt that the nodule was slowly growing and was now bothering her when wearing shoes. Her medical history was unremarkable, except for hyperthyroidism. Inspection of the patient’s left leg revealed no abnormalities of skin, bone, or muscle. No discoloration or signs of inflammation were noted on the skin over the nodule. On palpation, the nodule remained as a firm, subcutaneous, well-demarcated lesion. It was not fused to the skin or skeletal structures. No bone involvement or destruction was noted on radiology (Figure 1). The lesion was resected and referred to pathology.

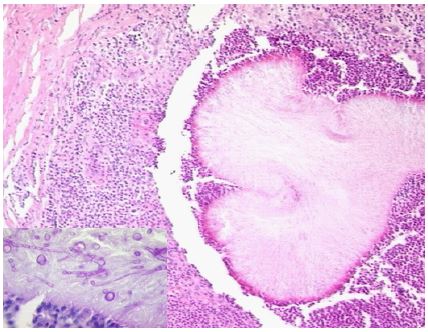
Histology revealed confluent foci of inflammation in the subcutis with reticulo-histiocytic inflammatory infiltrate and abscess formation, necrosis, and calcification. PAS-stain showed multiple septate and branched hyphae consistent with deep mycosis. Based on the histologic findings, infection with domestic fungal species was considered unlikely, and the possibility of tropical fungal infection was considered (Figure 2). Histology did not reveal the fungal species; therefore, molecular tests were performed on the paraffin-embedded tissue. After DNA extraction, amplification, and sequencing of the ITS2-region of its rDNA, Fusarium solani was identified, leading to the diagnosis of eumycetoma.
After surgery, no further pathological findings were observed from examination and imaging. Since the lesion had been completely resected, no antifungal medication was given. Over the course of two years, the patient underwent regular clinical examinations with no evidence of disease recurrence.
Conclusion
Our diagnosis of mycetoma is unusual, since the patient had no history of traveling to either Korea or tropical areas in recent years. Most likely, she contracted Fusarium solani in Germany through an injury while working in her garden. No fistula was present at the time of diagnosis. The patient had visited her physician in the early stages of the disease, which is not always possible for patients in rural tropical areas.
Fusarium species occur worldwide in nature and cause diseases like fungal keratitis, secondary infections of the skin, eumycetomas and in a setting of neutropenia, systemic mycosis. They can produce mycotoxins [7,8]. On histology, the hyphae of Fusarium solani resemble those of aspergillus. It is usually difficult to identify the fungal species by histology because morphological characteristics are nonspecific. Retrospective studies over ten years revealed a misinterpretation by histology in 21% of the cases [9]. A broad spectrum of fungal organisms can cause subcutaneous mycosis [10]. However, correct identification of the causing organism is necessary for adequate anti-mycotic treatment. Identification of the organism is possible through cultures as well as cytologic or histologic diagnosis with molecular studies, such as DNA-sequencing [11].
Unlike bacterial infections and actinomycotic mycetoma, which can be treated with systemic antibiotics, treatment of eumycetoma depends upon the progression of the disease and the infecting organism. Antibiotic or surgical treatment is possible, as well as a combination of both. In literature, treatment with trimethoprim-sulfamethoxazole is discussed for actinomycotic mycetoma, for eumycetomas, itraconazol and ketoconazol are treatment options, depending on the organism [6,13]. Small eumycetomas, like in our case, can be treated surgically (Welsh-method, [14]). When considering therapeutic options, superinfection or involvement of bone should be excluded.
Declarations
Acknowledgements: We thank Dr. Jürgen Bohl, Department of Neuropathology, J. Gutenberg University, Mainz, for advice and assistance; Dr. Kathrin Tintelnot, Division of Mycology, Robert Koch-Institut, Berlin, for performing molecular analysis.
Consent to participate, consent of publication: The involved patient agrees with participation and publication, a written consent form is available.
Declarations: The authors received no financial support or funding for the research, authorship, and/or publication of this article. The authors declare that they have no competing interests.
References
- Lichon V, Khachemoune A. Mycetoma: a review. Am J Clin Dermatol. 2006; 7(5): 315-21.
- Venkatswami S, Sankarasubramanian A, Subramanyam S. The madura foot: looking deep. Int J Low Extrem Wounds. 2012; 11(1): 31-42.
- Wang R, Yao X, Li R. Mycetoma in China: A Case Report and Review of the Literature. Mycopathologia. 2019; 184(2): 327-334.
- Cardenas-de la Garza JA, Welsh O, Cuellar-Barboza A, Suarez-Sanchez KP, Cruz-Gomez LG, et al. Climate, soil type, and geographic distribution of actinomycetoma cases in Northeast Mexico: A cross-sectional study. PLoS One. 2020; 15(5): e0232556.
- Hassan R, Simpson H, Cano J, Bakhiet S, Ganawa E, et al. Modelling the spatial distribution of mycetoma in Sudan. Trans R Soc Trop Med Hyg. 2021; 115(10): 1144-1152.
- Sampaio FMS, Wanke B, Freitas DFS, Coelho JMCdO, Galhardo MCG, et al. Review of 21 cases of mycetoma from 1991 to 2014 in Rio de Janeiro, Brazil. PLoS Negl Trop Dis. 2017; 11(2): e0005301.
- Dignani MC, Anaissie E. Human fusariosis. Clin Microbiol Infect. 2004; 10 Suppl1:67-75.
- Nenoff P, Bernhardt A, Tintelnot K, Kingreen V, Dücker P, et al. Cutaneous infection due to Fusarium oxysporum in a female diabetic: molecular biological detection of the mold from formalin-fixed paraffin embedded tissue using sequencing of the ITS region of the rDNA. Hautarzt. 2014; 65(6): 542-7.
- Sangoi AR, Rogers WM, Longacre TA, Montoya JG, Baron EJ, et al. Challenges and pitfalls of morphologic identification of fungal infections in histologic and cytologic specimens: a ten-year retrospective review at a single institution. Am J Clin Pathol. 2009; 131(3): 364-75.
- Nenoff P, van de Sande WWJ, Fahal AH, Reinel D, Schöfer H. Eumycetoma and actinomycetoma - an update on causative agents, epidemiology, pathogenesis, diagnostics and therapy. J Eur Acad Dermatol Venereol. 2015; 29(10): 1873-83.
- Bernhardt A, de Boni L, Kretzschmar HA, Tintelnot K. Molecular biological identification of fungal pathogens in FFPE tissue from cases of cephalic mycosis. Pathologe. 2013; 34(6): 504-7.
- Bernhardt A, von Bomhard W, Antweiler E, Tintelnot K. Molecular identification of fungal pathogens in nodular skin lesions of cats. Medical Mycology. 2015; 53(2): 132-44.
- Elkheir LYM, Haroun R, Mohamed MA, Fahal AH. Madurella mycetomatis causing eumycetoma medical treatment: The challenges and prospects. PLoS Negl Trop. Dis. 2020; 14(8): e0008307.
- Welsh O, Salinas MC, Rodríguez MA. Treatment of eumycetoma and actinomycetoma. Curr Top Med Mycol. 1995; 6: 47-71.