
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Emphysematous pyelonephritis with pleuro-pulmonary and
bladder involvement in a 30 year old diabetic woman: A case
of successful medical management
Ronald Gobina1,2 *; Teuwafeu Denis1,2; Nkuonlack Cyrille1,2; Nkoke Clovis1,2; Martin Mokake1,2; Fouda Hermine3,4; Kaze Folefack4,5; Ashuntantang Gloria5,6,7
1Buea Regional Hospital, Cameroon.
2Faculty of Health Sciences, University of Buea, Cameroon.
3Faculty of Medicine and Pharmaceutical Sciences, University of Douala, Yaounde, Cameroon.
4Faculty of Medicine and Biomedical Sciences, University of Yaounde, Cameroon.
5University Teaching Hospital, Cameroon.
6Faculty of Health Sciences, University of Bamenda, Cameroon.
7Yaounde General Hospital, Cameroon.
*Corresponding Author : Ronald Gobina
Buea Regional Hospital, Cameroon.
Faculty of Health Sciences, University of Buea, Cameroon.
Tel: +237699571640;
Email: ronaldgobina01@gmail.com
Received : Feb 21, 2023
Accepted : Apr 06, 2023
Published : Apr 13, 2023
Archived : www.jcimcr.org
Copyright : © Gobina R (2023).
Abstract
Emphysematous pyelonephritis (EPN) is a rare, severe, necrotizing renal parenchymal infection that is characterized by the production of intra-parenchymal gas and is most common in diabetics and in females. We describe a 30 year old woman with poorly controlled type 1 diabetes mellitus who presented with CT-confirmed left emphysematous pyelonephritis with concomitant emphysematous cystitis and bilateral pleural effusion with band atelectasia at the left lung base. She had clinical and laboratory signs of systemic inflammatory response syndrome and her urine culture isolated Proteus mirabilis as causative agent. She responded well to broad-spectrum antibiotics without percutaneous drainage or nephrectomy. Renal function remained normal throughout. Emphysematous pyelonephritis with concomitant emphysematous cystitis, bilateral pleural effusion and atelectasis is rare. Ultrasound and computerized tomography imagining is diagnostic of emphysematous disease as it shows presence of air in the renal parenchyma and the urinary bladder. Prompt medical management helps to reduce morbidity and mortality.
Keywords: Emphysematous pyelonephritis; Diabetes; Emphysematous cystitis.
Citation: Gobina R, Denis T, Cyrille N, Clovis N, Mokake M , et al. Emphysematous pyelonephritis with pleuro-pulmonary and bladder involvement in a 30 year old diabetic woman: A case of successful medical management. J Clin Images Med Case Rep. 2023; 4(4): 2370.
Introduction
Emphysematous Pyelonephritis (EPN) is a rare, severe, necrotizing renal parenchymal infection that is characterized by the production of intraparenchymal gas [1]. The combined occurrence of EPN with emphysematous cystitis and pleural effusion with atelectasis is uncommon.
Case
We report the case of a 33 year old woman who has a past history of type 1 diabetes mellitus. She was on insulin and had been non-compliant to treatment resulting in chronic hyperglycemia and recent glycated hemoglobin of 12.4%. She presented with a 3 weeks history of intermittent generalized abdominal pain and low grade fever. The pain was maximal at the left flank, gnawing in character, radiating towards the groin, initially mild but became severe by the second week of illness to an intensity of about 8/10. This was associated with nausea, vomiting, severe generalized weakness. Diuresis was conserved but urine was cloudy. There was pain during micturition, urinary frequency and urgency. On physical examination she was fully conscious and alert but looked very ill and was lethargic. Her vital signs were as follows: temperature 38.3oC, Blood pressure 98/75 mmHg, pulse 98 bpm, respiratory rate 26 cpm. Her abdomen was distended with a bulge at the left flank. The left kidney was palpable and very tender. Her urine was cloudy with a column of pus forming after standing for few hours.
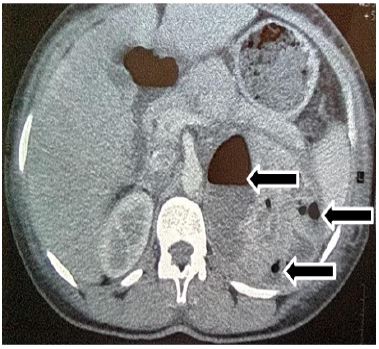
Renal ultrasound findings showed an enlarged left kidney of 170 mm in length, with a heterogeneous area of 68 mm at the upper pole containing multiple air bubbles and a hypoechoic collection. The right kidney measured 112 cm in length and had a normal parenchymal appearance. Computerized Tomography (CT) imaging of the abdomen showed an enlarged left kidney with several collections at the upper and middle poles, the largest being 60 mm wide and containing an air-fluid level. Renal secretion and excretion of contrast was symmetrical and within normal limits. There was an air fluid level in the urinary bladder and air bubbles within the bladder wall and at the bladder neck. The lower chest showed basal lung ground-glass opacity with a sub-pleural band of atelectasis and bilateral pleural effusion. Laboratory investigations at diagnosis are shown in Table 1 below.
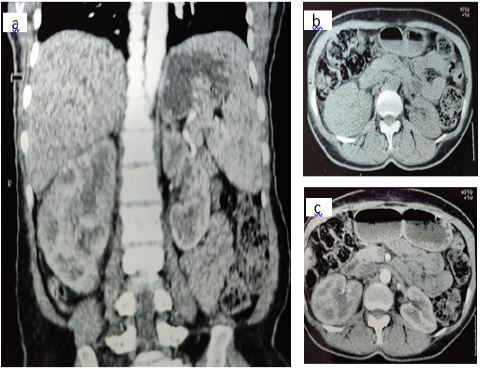
Her findings were compatible with emphysematous pyelonephritis of the left kidney, emphysematous cystitis and bilateral pleural effusion with a sub-pleural band of left lung basal atelectasis. She was hospitalized and treated with parenteral antibiotics consisting of Gentamycin for 5 days; plus Ceftriaxone and Metronidazole for 14 days each, followed by oral antibio therapy with Cefixim for 10 days. She also received IV fluids, parenteral Tramadol and Paracetamol and was placed on insulin. Progress was marked by complete regression of presenting signs and symptoms by the 2nd week of treatment, and normalization of laboratory markers of sepsis. Radiologic follow-up was done with ultrasound and showed normal sized kidneys by the 4th week but with the left kidney still presenting few gas bubbles. She continued with Levofloxacin for 10 days and remained asymptomatic until the 10th week when all radiologic lesions were shown to have disappeared. Renal function remained normal throughout her illness. One year later a repeat CT scan was done confirming absence of intra-parenchymal gas, and showed markedly enlarged right kidney (131 mm) while the left kidney length was (105 mm). Both kidneys had normal contrast uptake and excretion on CT scan. Renal function at 1 year was normal (Creatinine: 1.0 mg/dl) and dipstix was negative for proteinuria.
Table 1: Laboratory investigations at diagnosis.
| Laboratory test | Results | |
|---|---|---|
| Urine culture | Proteus mirabilis | |
| Leucocytes 3+ | ||
| Nitrites (+) | ||
| Proteins 1+ | ||
| Dipstix | Glucose 3+ | |
| Urine analysis | Blood 3+ | |
| S.G: 1.020 | ||
| pH: 6 | ||
| Culture | Proteus spp | |
| Serum Creatinine | 0.8 mg/dl | |
| Urea | 45 mg/dl | |
| Random Blood Sugar | 345 mg/dl | |
| Full blood Count | White cell count | 10600 cells/mm3 |
| Neutrophils | 8900 cells/mm3 | |
| Lymphocytes | 1200 cells/mm3 | |
| Hemoglobin | 9.2 g/dL | |
| Platelet count | 310000 cells/mm3 | |
| C reactive protein | 192 mg/dl | |
| HIV | Rapid Diagnostic test | negative |
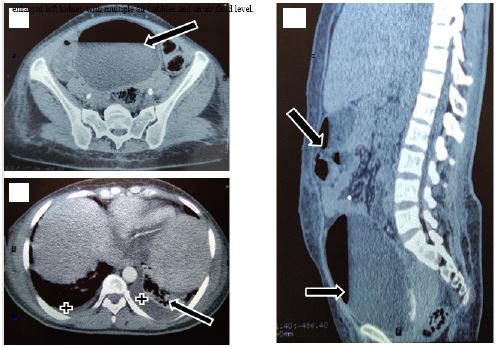
a) Emphysematous cystitis. Observe the air-fluid level within the urinary bladder (arrow).
b) Bilateral pleural effusion (crosses) with left basal atelectasis (arrow).
c) Arrows from top to bottom: emphysematous pyelonephrtitis, and emphysematous cystitis.
Discussion
Diabetes mellitus is the single most common factor associated with EPN, as up to 95% of patients with EPN have underlying uncontrolled diabetes mellitus [2,3]. The second most common risk factor is the female sex with reports of female predominance of 3:1 and up to 14:1 [2,4,5]. The hyperglycemic environment in known to inhibit leucocyte function thereby impairing response to infections [2,6] and in females, a higher incidence of asymptomatic bacteriuria of up to 26% compared to 6% in non-diabetic females [7] further increases the risk of pyelonephritis. Proteus mirabilis alongside Escherichia coli and Klebsiella pneumonia are among pathogens known to cause mixed acid fermentation, a process postulated to explain gas formation consisting mainly of H2 and C02 within infected renal tissue [8,9]. The association of emphysematous cystitis and EPN, although uncommon, is known [10] and a similar case of bilateral pleural effusion with band atelectasis of the left lung base has also been reported [9]. Concomitant involvement of the kidney and bladder may be explained by ascending or descending infection and extension of infection from EPN to the adjacent subcutaneous tissue in the abdomen or chest has been proposed [11]. Treatment options of EPN include Medical Management (MM) alone, Percutaneous Drainage (PCD) plus MM, MM plus emergency nephrectomy and MM plus PCD plus emergency nephrectomy [12]. Whereas medical management alone has mortality rate of about 50%, MM plus PCD lowers mortality to 13.5% [12] and some authors recommend PCD as the most appropriate management strategy for most patients and CT-guided PCD as the modality of choice [1,2]. For logistic and socioeconomic reasons our patient had access to MM only and radiologic follow-up was done with ultrasound. Conservative management however, is increasingly being employed with good results [3,13,14] as our case illustrates. Unilateral nephromegaly has been associated with several factors including kidney scarring in children following a first episode of urinary tract infection and compensatory hypertrophy from contralateral renal disease [15-17]. Our patient developed unilateral nephromegaly following a severe urinary tract infection and although her serum creatinine levels remained normal throughout the infectious episode, the extent of left kidney involvement by the EPN suggests some level of renal parenchymal destruction. Partial parenchymal destruction with normal serum creatinine is not unusual as remnant nephrons are able to adapt to maintain normal serum creatinine levels even when as much as one whole kidney is rendered non- functional by disease or removal, these apparent normal serum creatinine levels however, being a poor predictors of GFR [18-21]. Overt structural changes on the other hand may take time to install and the gross asymmetry in the kidney sizes in our patient may reflect changes whose induction started one year earlier during the PRN episode. Long term monitoring will be required to track function and further structural changes to the kidneys as the case may be.
Conclusion
Emphysematous pyelonephritis with concomitant emphysematous cystitis, bilateral pleural effusion and atelectasis is rare. CT is diagnostic of emphysematous disease as it shows presence of air in the renal parenchyma and the urinary bladder. Prompt medical management helps to reduce morbidity and mortality.
References
- Ubee SS, McGlynn L, Fordham M. Emphysematous pyelonephritis: Emphysematous pyelonephritis. BJU Int. 2011; 107: 1474–1478.
- Pontin AR, Barnes RD. Current management of emphysematous pyelonephritis. Nat Rev Urol. 2009; 6: 272–279.
- Elawdy MM, Osman Y, Abouelkheir RT, El-Halwagy S, Awad B, El-Mekresh M, et al. Emphysematous pyelonephritis treatment strategies in correlation to the CT classification: Have the current experience and prognosis changed? Int Urol Nephrol. 2019; 51: 1709–1713.
- Baliga KV, Narula AS, Sharma A, Khanduja R, Manrai M, et al. Successful Medical Treatment of Emphysematous Pyelonephritis in a Renal Allograft Recipient. Ren Fail. 2007; 29: 755–758.s
- Shokeir AA, El-Azab M, Mohsen T, El-Diasty T. Emphysematous pyelonephritis: A 15-year experience with 20 cases. Urology. 1997; 49: 343–346.
- Jafar N, Edriss H, Nugent K. The Effect of Short-Term Hyperglycemia on the Innate Immune System. Am J Med Sci. 2016; 351: 201–211.
- Stapleton A. Urinary tract infections in patients with diabetes. Am J Med. 2002; 113: 80–84.
- Huang JJ, Tseng CC. Emphysematous pyelonephritis: Clinicoradiological classification, management, prognosis, and pathogenesis. Arch Intern Med. 2000; 160: 797–805.
- Khaladkar SM, Jain KM, Kuber R, Gandage S. Necrotizing Fasciitis of Thoracic and Abdominal Wall with Emphysematous Pyelonephritis and Retroperitoneal Abscess. J Clin Imaging Sci [Internet]. 2018; 8. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5843965/
- Li S, Wang J, Hu J, He L, Wang C, et al. Emphysematous pyelonephritis and cystitis: A case report and literature review. J Int Med Res. 2018; 46: 2954–2960.
- Ishigami K, Bolton-Smith JA, Deyoung BR, Barloon TJ. Necrotizing fasciitis caused by xanthogranulomatous and emphysematous pyelonephritis: Importance of the inferior lumbar triangle pathway. AJR Am J Roentgenol. 2004; 183: 1708–1710.
- Somani BK, Nabi G, Thorpe P, Hussey J, Cook J, N’Dow J, et al. Is Percutaneous Drainage the New Gold Standard in the Management of Emphysematous Pyelonephritis? Evidence From a Systematic Review. J Urol. 2008; 179: 1844–1849.
- Bhat RA, Khan I, Khan I, Palla N, Mir T, et al. Emphysematous pyelonephritis: Outcome with conservative management. Indian J Nephrol. 2013; 23: 444–447.
- Tchokouaha FN, Etoa M, Ashuntantang G. P29 Severe renal failure in a diabetic patient with urinary tract infection: The kidney may be in bubbles! Diabetes Res Clin Pract. 2014; Supplement 1: S41.
- Cheng CH, Hang JF, Tsau YK, Lin TY. Nephromegaly is a Significant Risk Factor for Renal Scarring in Children With First Febrile Urinary Tract Infections. J Urol. 2011; 186: 2353–2358.
- Dossetor RS. Renal compensatory hypertrophy in the adult. Br J Radiol. 1975; 48: 993–995.
- Dm RC, Jy L, L M, Jm G. Compensatory renal hypertrophy following nephrectomy: When and how? Nephrol Carlton Vic [Internet]. 2019; 24. Available from: https://pubmed.ncbi.nlm.nih.gov/30809888/
- Tan JC, Ho B, Busque S, Blouch K, Derby G, Efron B, Myers BD, et al. Imprecision of Creatinine-Based GFR Estimates in Uninephric Kidney Donors. Clin J Am Soc Nephrol. 2010; 5: 497.
- Kaplan B, Schold J, Meier-Kriesche HU. Poor predictive value of serum creatinine for renal allograft loss. Am J Transplant Off J Am Soc Transplant Am Soc Transpl Surg. 2003; 3: 1560–1565.
- Chopra B, Sureshkumar KK. Limitation of Terminal Serum Creatinine as a Kidney Donor Profile Index Variable in Predicting Long-Term Kidney Transplant Outcomes. Transplant Proc. 2018; 50: 1272–1275.
- Duru OK, Vargas RB, Kermah D, Nissenson AR, Norris KC, et al. High prevalence of stage 3 chronic kidney disease in older adults despite normal serum creatinine. J Gen Intern Med. 2009; 24: 86–92.