
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Trevor disease (Dysplasia Epiphysealis Hemimelica)
in children: A case report
Khaled Anis Kamoun1*; Achref Ferjani1; Seifeddine Mahjoubi1; Wajdi Arfa1; Faten Farah2; Mourad Jenzri1
1Pediatric Orthopedic Surgery Department, Kassab Institute, El Manar University, Tunisia.
2Anatompathology Department, Kassab Institute, El Manar University, Tunisia.
*Corresponding Author : Khaled Anis Kamoun
Associate Professor, Pediatric Orthopedic Department, Kassab Orthopedic Institute, Elmanar University, Tunis, Tunisia.
Phone:(+216)20062345;
Email: kamounkhaledanis@gmail.com
Received : Mar 20, 2023
Accepted : Apr 10, 2023
Published : Apr 17, 2023
Archived : www.jcimcr.org
Copyright : © Kamoun KA (2023).
Abstract
Dysplasia Epiphysealis Hemimelica (DEH) or Trevor disease is a condition that affects skeletal development characterized by asymmetric abnormal growth in epiphyses cartilage. Clinical signs are uncommon and variable; resulting in a non standardized treatment approach. We reported a case of a 13-year-old child complaining from left knee pain and swelling of the medial side. X-ray showed overgrowth of mass extruding from the femoral medial epiphysis. MRI images demonstrate a heterogeneous fragment with well defined epiphysis separation and bone edema. All these imaging reminds DEH. Surgery was performed through a medial approach to excise the articular cartilaginous mass. The mass arose from the articular epiphysis. The excised mass demonstrated cartilaginous caps over the bones and histological study showed fibro-osseous proliferation under a chondral cap and enchondral ossification. After surgery, the limb was protected by above knee spica for 14 days followed by partial weight-bearing. The patient recovered rapidly after several rehabilitation sessions. No recurrence reported at follow up.
Even if our case has a good outcome, prognosis of such disease can be unpredictable and largely depends on the size and location of the affected area. And only symptomatic lesions or those that impact function should be treated surgically.
Keywords: Hemimelic epiphyseal dysplasia; Trevor disease; Epiphysis.
Citation: Kamoun KA, Ferjani A, Mahjoubi S, Arfa W, Farah F, et al. Trevor disease (Dysplasia Epiphysealis Hemimelica) in children: A case report. J Clin Images Med Case Rep. 2023; 4(4): 2374.
Introduction
Hemimelic Epiphyseal Dysplasia (HED), or Trevor disease, is a rare skeletal disorder characterized by asymmetric cartilage growth in one or more epiphyses [1]. Its etiology is unknown, but may relate to epiphysis blood flow disturbance [2]. It affects male patients three times more often than females (3:1 ratio) [3,4]. Histologically, the lesion is indiscernible from an osteochondroma. The location is typically hemimelic, with focal overgrowth of the medial (most frequently) or lateral portion of the epiphysis. The first report dates back to 1926, where it was described as tarsomegaly [5].
Trevor [2] reported the first 8 cases in the English language literature. In 1956, Fairbank [1] gave the term “dysplasia epiphyseal is hemimelica”, which is still used today. Due to the variability of the presentation, there is no standardized treatment. The aim of this case presentation is to report an additional case and to review the literature with main attention to the treatment and prognosis of the disease.
Case presentation
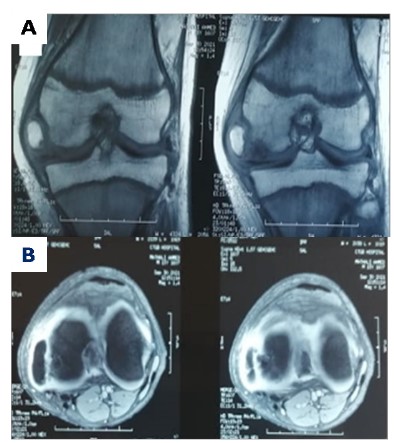
A 13 years old boy with no relevant medical history was first seen in outpatient department for progressive appearance of a tumor in the medial region of the left knee. He reported little pain and limping. Physical exam showed full range of knee motion, with no limb length discrepancy or imbalance. Neurovascular examination was normal. Initial radiographs showed an overgrowth of mass extruding from the femoral medial epiphysis suggesting a benign lesion (Figure 1). MRI demonstrates a heterogeneous mass arising from medial epiphysis with well defined separation and bone edema (Figure 2a-b). According to radiologist report all these imaging reminds Trevor disease.
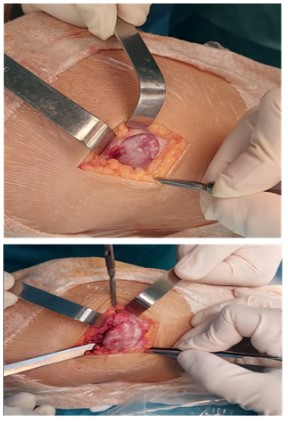
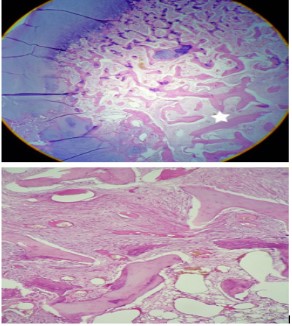
The child remains symptomatic even without any sport activities this is why surgery was performed through the medial approach to excise the articular cartilaginous mass. This mass arose from the articular epiphysis. Spatula and bone chisel was used to dissociate it from epiphysis (Figure 3a-b). The fragment excised size was 3 x 1.5 cm, with bone covered by cartilaginous cap sent for anatomopathological analysis (Figure 4). Histological findings confirmed diagnosis showing fibro-osseous proliferation, cartilaginous cap and enchondral ossification (Figure 5a-b).


After surgery, the limb was protected by above knee spica for 14 days followed by partial weight-bearing. The patient recovered rapidly after several rehabilitation sessions. No recurrence reported at follow up.
Discussion
Etiopathogeny of DEH is currently unknown, and there is no evidence to support genetic inheritance. It is believed that DEH is a congenital developmental disorder affecting the pre- or postaxial lower limb due to the involvement of the apical ectodermal cap [1]. Treatment options depend on the location and severity of symptoms and may include observation, surgical resection, or corrective osteotomies. Early surgery is recommended for cases with intraarticular masses to prevent damage to the articular cartilage and secondary osteoarthritis. In cases where there is articular incongruity, early surgery is also recommended. However, Kuo et al. have reported recurrence of DEH and fixed deformity in intraarticular cases [6]. Unlike dysplasia epiphysialis punctata, where the entire width of the epiphysis is affected, only one half of the epiphysis is affected in DEH [2]. The distribution of cells and vessels within the epiphysis explains the pattern of DEH, according to Trevor [2]. Bhosale described the cocarde-like design of the epiphysis, where the center is formed by a bony trabecula of the ossific nucleus. The degenerated cartilaginous cells are arranged in columns around it, and between this layer and the mitotic annulus, which is the outermost layer, there is a zone consisting of the youngest cartilaginous cells [7]. The surface cells are old and flat, becoming a component of the synovial fluid as they deteriorate. However, in DEH, these cells do not become senile and remain capable of division, forming multiple masses of cartilage with areas that later calcify.
Patients with this disorder typically present with pain, limited range of motion, and noticeable deformity [1]. Varus and valgus deformities are common, as is the presence of a mass. The deformities tend to worsen as the patient grows, but the condition is self-limited by the closure of the epiphysis at puberty [8,9].
A simple radiograph can be useful in diagnosing DEH. The massive ossification of the hypertrophic cartilage leads to degenerative changes in the affected joints at a high rate, resulting in arthritis. Multiple independent ossification centers can be seen around the epiphyses on radiographic images. Differential diagnosis may include post traumatic bone fragment, synovial chondromatosis, osteochondroma, aneurysmal bone cyst, and even chondroblastoma [10]. Most cases of DEH reported in the literature have been treated surgically by resecting the tumor and correcting the deformity while preserving the integrity of the joint surfaces. Untreated cases can result in angular deformity, limb length discrepancies, and early degenerative arthritis. Gökkus et al. reported four cases of Trevor’s disease involving the ankle in 2016, all of which were treated by completely resecting the osteochondromas with no recurrence reported, allowing the patients to return to their previous physical activities [11]. Following surgery, there is a possibility of limb overgrowth due to increased blood flow to the affected area. However, limb shortening may occur if there is premature physis closure resulting from the disease or as a iatrogenic complication. [11]. Nishiyama et al. [12] achieved a favorable outcome after performing osteotomy on a 12-year-old female patient who had reached the end of her growth period. Azouz et al. [13] recommend surgery whenever there is a need to correct deformity or restore function, but they also noted that there is a risk of abnormal bone growth and local vasculature stimulation in severe cases. However, malignant degeneration has not been reported. Regular follow-up is necessary until skeletal maturity, regardless of the subtype of the disease. Azzoni [14] uses the terms juxta-articular and articular because most lesions are found inside the joint capsule, and they consider tumors outside the joint capsule as extracapsular. Asymptomatic patients with intra-articular involvement may be observed without surgery, as early surgery may lead to osteoarthritis. Depending on the clinical presentation of the tumor, asymptomatic patients may not require any medical intervention, as there have been no reports of malignant transformation. In cases where there is a painful deformity or functional impairment due to DEH, surgical excision may be an option in extracapsular cases to improve joint congruity. Intra-articular lesions that have the potential to recur require a more complex surgical technique [15].
Conclusion
Even if DEH treatment is not clearly defined in the literature, symptomatic lesions or those that interfere with function should be treated surgically. The prognosis is variable and depends basically on its location and size. Patients’ undergone surgery should be followed periodically because of the risk of recurrence.
Ethics consideration: The patient and family were informed that data on the case would be submitted for publication. Consent was signed prior to the preparation of the manuscript.
References
- Fairbank TJ. Dysplasia epiphysealishemimelica (tarsoepiphysial- aclasis). J Bone Joint Surg (Br). 1956; 38: 237-257.
- Trevor D. Tarso-epiphysial aclasis. J Bone Joint Surg (Br). 1950; 32B: 204-213.
- Skaggs DL. Moon CN. Kay RM. Peterson, H.A. Dysplasia Epiphysealis Hemimelica of the Acetabulum. A report of two cases. J. Bone Jt. Surg. Am. 2000; 82: 409–414.
- Schmale GA, Conrad EU III; Raskind WH. The natural history of hereditary multiple exostoses. J. Bone Jt. Surg. Am. 1994; 76: 986–992.
- Mouchet A, Belot J. La tarsomegalie. J Radiol Electrol. 1926; 10:289-293.
- Kuo RS, Bellemore MC, Monsell FP, Frawley K, Kozlowski K. Dysplasia Epiphysealis Hemimelica: Clinical Features and Management. J. Pediatr. Orthop. 1998; 18: 543–548.
- Bhosale SK, Dholakia DB, Sheth BA, Srivastava SK. Dysplasia Epiphysealis Hemimelica of the Talus: Two Case Reports. J. Orthop. Surg. 2005; 13: 79–82.
- Kettelkamp DB, Campbell CJ, et al. Dysplasia epiphysealishemimelica: A report of fifteen cases and a review of the literature. J. Bone Joint Surg. 1966; 48-A: 746–765.
- Keats T. Dysplasia epiphysialishemimelica (tarso-epiphysial aclasis). Radiology. 1957; 68: 558–563,
- Nair AV, Anirudh S. Unusual presentation of chondroblastoma mimicking Trevor’s disease. J. Postgrad. Med. 2017; 63: 273.
- Gokkus K, Atmaca H, Sagtas E, Saylik M, Aydin AT. Trevor’s disease: Up-to-date review of the literature with case series. J Pediatr. Orthop B. 2017; 26: 532–545.
- Nishiyama M, Nii E, Akeda K, Uchida A. Limb-lengthening and angular correction for dysplasia epiphysealishemimelica. J. Orthop. Sci. 2001; 6: 358–361.
- Azouz EM, Slomic AM, Marton D, Rigault P, Finidori G. The variable manifestations of dysplasia epiphysealishemimelica. Pediatr. Radiol. 1985; 15: 44–49.
- Azzoni R. Dysplasia epiphysealishemimelica of the talus. J. Orthop. Traumatol. 2009; 10: 43–46.
- Jovanovic DV, Ili MB, Mihajlovic MZ, Vojinovi´c RH, Mitrovic SL, et al. Dysplasia epiphysealishemimelica: A case report. Vojnosanit. Pregl. 2014; 71: 1081–1084.