
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Encapsulated papillary carcinoma without concurrent
breast cancer in an axillary lymph node
Kevin Toolan*; Carter Do; Ankica Braun; Paolo Gattuso; Rosalinda Alvarado
Department of Surgery, Department of Pathology, Rush University Medical Center, USA.
*Corresponding Author : Rosalinda Alvarado
Department of Surgery, Department of Pathology,
Rush University Medical Center, USA.
Email: rosalinda_alvarado@rush.edu
Received : Mar 20, 2023
Accepted : Apr 12, 2023
Published : Apr 19, 2023
Archived : www.jcimcr.org
Copyright : © Alvarado R (2023).
Abstract
We report a case of encapsulated papillary carcinoma arising de novo in an axillary lymph node. This rare diagnosis is thought to occur via epithelial rest. Our case is suggestive of epithelial rest playing a role in our patient’s pathogenesis.
Keywords: Breast malignancy; Papilloma; Cancer; Axillary lymph node.
Citation: Toolan K, Do C, Braun A, Gattuso P, Alvarado R. Encapsulated papillary carcinoma without concurrent breast cancer in an axillary lymph node. J Clin Images Med Case Rep. 2023; 4(4): 2377.
Introduction
Papillary carcinoma is a rare type of invasive ductal carcinoma that typically does not metastasize to the lymph nodes. Even rarer is the presence of papillary carcinoma in the axillary lymph node without concurrent breast carcinoma. Only a few case reports highlight this phenomenon [1]. Two mechanisms were hypothesized: (1) cellular displacement of normal or pathologic breast tissue through surgical or needle manipulation or (2) embryonic malformation leading to epithelial rest in the lymph node [2]. We present a case of axillary lymph node papillary carcinoma in a patient with a history of intraductal papilloma and progressive axillary lymph node biopsy findings.
Case description
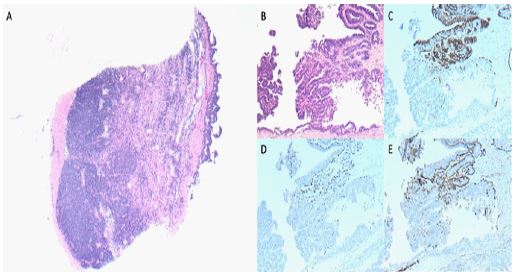
Our patient is a 65-year-old woman who presented to the breast surgeon to evaluate a right axillary mass. Her past medical history was significant for right intraductal papilloma without atypia (Table 1). Six years before presentation the patient was found to have intraductal papilloma without atypia. A biopsy of the right axillary lymph node at that time showed a benign reactive lymph node with a microscopic focus on epithelial inclusion. She remained stable for almost four years until she noticed a slow-growing lump over two years, prompting her to obtain a mammogram and ultrasound in March 2022. Her imaging revealed a 2.7 x 1.7 x 2.6 cm cystic right axillary nodular mass with septation, eccentric wall thickening, and internal vascularity. On exam, the lump was non-tender, non-fluctuant and mobile. She underwent a core needle biopsy (CNB) of the axillary mass. Pathology revealed intraductal papillary neoplasm with associated atypia. A portion of lymphoid tissue was adjacent to the papillary lesion presence of germinal centers and a capsule, which represents a portion of a lymph node. Immunohistochemical stains showed loss of staining for cytokeratin 5 and smooth muscle actin, whereas estrogen receptors showed strong diffuse staining (Figure 1). Excision of the lesion was recommended to rule out ductal carcinoma in situ (DCIS). The follow-up excision demonstrated an atypical papillary lesion with monomorphic cells showing low-grade nuclear atypia (Figure 2). Immunohistochemical stains for CK5, SMMS, and p63 showed loss of staining for myoepithelial cells both within the fibrovascular cores and at the periphery of the lesion. Based on these findings, a diagnosis of encapsulated papillary carcinoma arising in an intraductal papilloma within a lymph node was rendered. Although a portion of benign papilloma was identified in the biopsy specimen, no residual benign papilloma was present. The presence of benign epithelial inclusion was identified also in this specimen (Figure 1A). All margins were negative for DCIS (Table 1).
Table 1: Progression of right breast/axillary lymph node findings.
| Date | Test | Sample | Findings |
|---|---|---|---|
| (01/2015) | CNB | Breast (12:00) | Intraductal papilloma w/o atypia; ER+ (>90%); p63+ |
| (07/2015) | FNA | Breast cystic fluid | Benign, consistent with abscess |
| CNB | Axillary LN | Benign lymph node; microscopic focus of benign epithelial inclusion | |
| (01/2016) | FNA | Axillary LN | Reactive lymph node; predominately small lymphocytes and few lympho-histiocytic groups |
| (02/2016) | Post-Op Path Report | Breast (12:00) | Intraductal papilloma w/o atypia; ER+ (>90%); p63+, cytokeratin5+ |
| Nipple (behind) | Benign breast tissue | ||
| (04/2022) | CNB | Axillary LN | Intraductal papilloma with atypical ductal hyperplasia. Apocrine metaplasia and dense lymphoid reaction. Florid lymphoid reaction. |
| (05/2022) | Post-Op Path Report | Axillary LN | Atypical papillary lesion, consistent with an encapsulated papillary carcinoma, nuclear grade 12, arising within a lymph node. ER+/PR+; p63 |
FNA: fine needle aspiration; CNB: core needle biopsy.

On 10-day follow-up, the patient underwent right axillary seroma aspiration and drain placement for persistent seroma. Total body bone and CT scans were negative for distant metastasis. She was started on Anastrozole. Adjuvant radiation therapy was not recommended.
Discussion
Our case demonstrates a rare presentation of papillary carcinoma in an axillary lymph node. The absence of concurrent breast carcinoma suggests an etiology that does not follow the characteristic mechanism of metastasis of cancer from the breast to the lymph nodes.
Bleisweiss et al. found that the friable nature of intraductal papilloma can make them prone to fragmentation, dislodgement, and passive transport to axillary lymph nodes [3,4]. While a reasonable hypothesis, it does not fit well with our case presentation given the initial breast biopsy was without atypia. In our case, we propose a different etiology for our patient’s pathology.
Benign epithelial inclusions were discovered in her CNB from 07/2015 and were also redemonstrated in the excision specimen from 5/2022. These cellular findings have been attributed to epithelial rests during embryonic development [1,3,5]. It is reasonable to conclude embryonic arrest followed by malignant transformation occurred independent of our patient’s breast pathology. Srinivasan et al. investigated the significance of benign epithelial inclusions in an axillary lymph node, concluding that these nodal inclusions developed into DCIS in their patient [3]. It is reasonable to apply this pathogenesis to our case because DCIS and papillary carcinoma share ductal tissue as tissue of origin.
We hypothesize that the epithelial cells within the axillary lymph node transformed into intraductal papilloma, developing into papillary carcinoma. This is supported by the presence of a portion of benign intraductal papilloma in the biopsy prior to the excision which showed encapsulated papillary carcinoma. The current literature suggests presence of ectopic breast tissue to be an incidental microscopic finding with unclear diagnostic significance. There are no recommendations for monitoring for proliferative changes in benign epithelial inclusions, likely due to the rarity of them becoming malignancies [6]. Despite the infrequency of de novo carcinomas developing in an axillary lymph node, pathologists and clinicians should be aware of the possible occurrence and proliferation that can take place.
We present a rare cancer and place it in the context of the current understanding of axillary cancer. Our study is limited by its retrospective nature; however, the significant number of biopsies should provide assurance that all important timepoints were captured in the pathogenesis of our patient’s cancer. Future studies, preferentially in a prospective manner, are warranted to further elucidate the pathogenesis and etiology of papillary carcinoma in axillary lymph nodes.
References
- Jaffer S, Lin R, Bleiweiss IJ, Nagi C. Intraductal carcinoma arising in intraductal papilloma in an axillary lymph node: Review of the literature and proposed theories of evolution. Archives of pathology & laboratory medicine (1976). 2008; 132(12): 1940-1942.
- Fellegara G, Carcangiu M, Rosai J. Benign epithelial inclusions in axillary lymph nodes: Report of 18 cases and review of the literature. The American journal of surgical pathology. 2011; 35(8): 1123-1133.
- Srinivasan B, Allan CP, Armes JE. Ductal carcinoma in situ arising in an epithelial inclusion within an axillary lymph node. Pathology. 2007; 39(2): 268-269.
- Bleiwess I, Nagi C, Jaffer S. Axillary sentinel lymph nodes can be falsely positive due to iatrogenic displacement and transport of benign epithelial cells in patients with breast carcinoma. Journal of clinical oncology. 2006; 24(13): 2013-2018.
- Maiorano E, Mazzarol GM, Pruneri G, Mastropasqua MG, Zurrida S, Oreito E, et al. Ectopic breast tissue as a possible cause of false-positive axillary sentinel lymph node biopsies. The American journal of surgical pathology. 2003; 27(4): 513-518.
- Cottom H, Rengabashyam B, Turton PE, Shaaban AM. Intraductal papilloma in an axillary lymph node of a patient with human immunodeficiency virus: a case report and review of the literature. J Med Case Rep. 2014; 8: 162.