
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 4
Incidental epileptic seizure findings on PET-CT: Case reports
Kaman Chung*; Gauke Klammers; Johnmh De Klerk
Department of Nuclear Medicine, Meander Medical Center, Amersfoort, the Netherlands.
*Corresponding Author : Kaman Chung
Department of Nuclear Medicine, Meander Medical Center, Amersfoort, the Netherlands.
Email: kaman.chung10@gmail.com
Received : Mar 22, 2023
Accepted : Apr 14, 2023
Published : Apr 21, 2023
Archived : www.jcimcr.org
Copyright : © Chung K (2023).
Abstract
Invasive surgery may be required to resect the area of the seizure in approximately one third of epilepsy patients. A combination of diagnostic tests is used to ascertain the resection area, including nuclear imaging (PET/SPECT) techniques that can accurately localize areas of seizures. Limited data is available on ictal PET-CT imaging, because PET-CT images are usually obtained in interictal phases and cannot be routinely obtained in the ictal phase because of logistic issues. This is in part due to the short decay period of FDG, which is a cyclotron produced radiopharmaceutical. Furthermore a fast uptake of FDG by the brain is preferable for imaging of ictal foci. Occasionally, ictal or early post-ictal phase findings are captured in patients undergoing whole body PETs for other medical purposes. We present two oncologic cases with incidental epileptic findings captured on PET-CT with FDG, visible as hypermetabolic areas in the brain. These cases highlight that when brain hypermetabolic foci are encountered on PET imaging in patients with a known carcinoma, the possibility of seizures aside from metastases needs to be taken into account.
Keywords: PET-CT; Epilepsy; Seizure; Hypermetabolism.
Abbreviations: BBB: Blood-Brain Barrier; CT: Computed Tomography; EEG: Electroencephalogram; FDG: 18f-Fluorodeoxyglucose; MRI: Magnetic Resonance Imaging; SPECT: Singlephoton Emission Computerized Tomography; PET: Positronemission Tomography.
Citation: Chung K, Klammers G, De Klerk J. Incidental epileptic seizure findings on PET-CT: Case report. J Clin Images Med Case Rep. 2023; 4(4): 2382.
Introduction
Epilepsy is a disorder characterized by recurrent brain seizures due to interrupted nerve cell activity. Treatment with anti-epileptic drugs can control seizures in most of the patients with epilepsy. However, in approximately one third of the patients invasive surgery may be required to resect the area of the seizure. For this group of patients, precise localization of the area of seizure is key to increase probability of successful outcomes of the surgical resection. To ascertain the resection area a combination of diagnostic tests including imaging is used. Image modalities such as MRI and nuclear imaging (PET/SPECT) are well established imaging techniques used to localize areas of seizures [1,2].
SPECT is a nuclear imaging technique that uses scintillation and Computed Tomography (CT) to detect photons generated from a radioactive tracer (e.g. 99m-Tc-HMPAO). The tracer is injected intravenously and the tracer perfusion of tissues and organs can be imaged on a SPECT-CT camera. The tracer can be taken up by the brain within a few minutes and therefore the injection can be performed right after the seizure (i.e. ictal phase) takes place to localize the affected area [2,3].
PET-CT is a higher quality 3D nuclear imaging technique that can be used to localize epileptic foci by using FDG (18F-Fluorodeoxyglucose) as a tracer. FDG is a glucose analogue that is actively transported across the Blood-Brain Barrier (BBB) and is then trapped within cells [2]. Ictal foci as well as early post-ictal foci up to 48 hours after the seizure are known to cause hypermetabolic areas [4]. Most interictal phase studies performed at a certain time point following a recent seizure typically demonstrate focal FDG hypometabolism [2,3]. However, the cause of this hypometabolism is not completely clear; neuronal loss or functional disturbance has been described as possible causes [5].
Because FDG is taken up by the brain in 30-45 minutes [3], PET-CT images for epilepsy are usually obtained in interictal phase and are not obtained in ictal phase for which a fast uptake by the brain is preferable. Furthermore there are logistic issues, in part due to the short decay period of FDG, which is a cyclotron produced radiopharmaceutical. Therefore limited data is available on ictal PET-CT imaging. Occasionally ictal or early post-ictal phase findings are captured in patients undergoing whole body PETs for other medical purposes.
We present two oncologic cases with incidental epileptic findings captured on PET-CT with FDG, visible as hypermetabolic areas in the brain.
Case presentations
Case 1
A 68-year old Caucasian female experiencing fatigue and a cough was referred to the Pulmonology outpatient department in 2022 because of an abnormal finding on chest X-ray suspicious for lung cancer. Given the suspicious findings on the chest X-ray a contrast enhanced upper body CT and FDG PET-CT was indicated for further investigation.
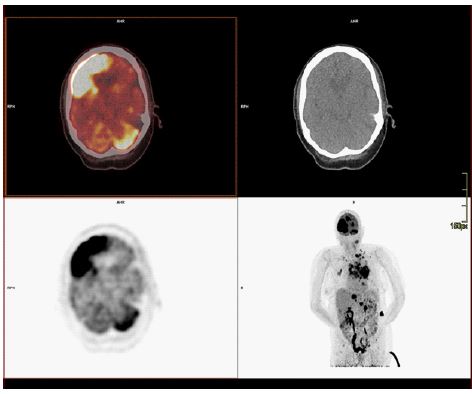
Imaging revealed a mediastinal mass extending into the lung left upper lobe, which showed increased FDG uptake on PET, highly suspicious for a primary lung carcinoma with extensive expansion into the mediastinum. Extensive metastatic bone and adrenal gland disease was found on PET. Furthermore, several hypermetabolic intracranial lesions were noted. The biggest lesion was located in the right frontal lobe with a maximum diameter of 7 cm. Another notable lesion was located in the left cerebellar hemisphere (Figure 1). These abnormal findings were initially interpreted as brain metastases, given the extensive metastatic disease found in other organs.
However, days later it was discovered that the patient had two brief unresponsive seizure episodes on the way to the PET scanner and had another episode on the ward after the PET examination. It was suspected that the seizures were caused by the brain metastases. Since Magnetic Resonance Imaging (MRI) is considered the standard for imaging metastatic brain cancer, MRI with contrast-enhancement was obtained subsequently to analyze the extensiveness of metastatic brain disease.
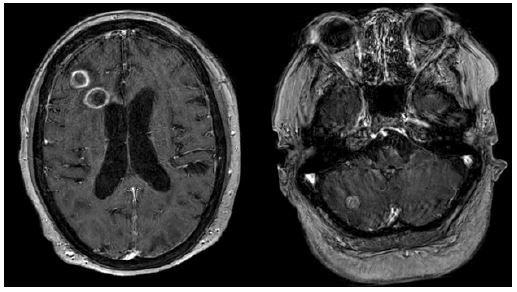
Consistent with the earlier PET-CT multiple brain metastases were found on MRI. However, not all lesions found on PET could be correlated with the brain MRI. The two most notable lesions seen on PET in the right frontal lobe and the left cerebellum could not be matched with MRI. There were small metastatic lesions in the right frontal lobe on MRI that did not match with the 7 cm lesion with high FDG-uptake on PET. Furthermore, on the brain MRI no lesion was found in the left cerebellum, while the whole left cerebellum showed FDG-uptake on the PET scan (Figure 2).
Thus, what we observed on PET-CT must have been findings of the epileptic seizure during or shortly after the seizure. We believe the findings found are consistent with frontal lobe epilepsy with contralateral cerebellar hypermetabolism, a rare phenomenon caught incidentally on PET-CT.
Case 2
A 48-year old male patient experienced symptoms of fatigue, fever and thirst for a period of time. Subsequently, he was diagnosed with diabetes mellitus by his general practitioner. He had been prescribed diabetes medication for a week, before presenting to the Emergency Room (ER) in our hospital due to diabetic ketoacidosis de novo triggered by an unknown cause.
During patient anamnesis at the ER the patient experienced a brief lapse of consciousness and was unresponsive. He was unresponsive for a short period of time and recovered fully after thirty seconds with no lingering confusion or other ill effects.
The differential diagnosis of diabetic ketoacidosis in this case mainly included a viral infection or malignancy. A CT was requested to investigate the cause of his diabetic ketoacidosis. A brain MRI was requested to check for any abnormalities causing the absence seizure.
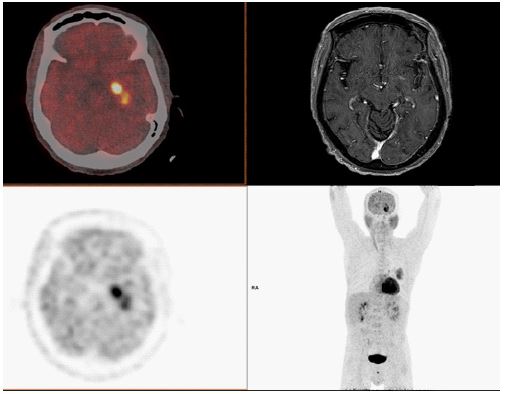
On CT a big mediastinal mass on the left side was found with extensive left-sided lymphadenopathy, consistent with a pulmonary malignancy. Subsequently a PET-CT was obtained for staging. The mediastinal mass and lymphadenopathy as seen on CT showed high FDG uptake. Multiple distant metastases were found in the liver, in the adrenal gland and in the skeleton. Furthermore, the PET-CT showed a focal area with high FDG avidity in the left mesial temporal lobe. A brain MRI was obtained four days earlier which showed no signs of brain metastasis (Figure 3). Therefore the FDG avid zone is believed to be consistent with a post-ictal area of hypermetabolism in the temporal area. However, the time period between the presentation in the ER and the PET-CT was 6 days, thus this likely concerned another seizure not objectified by physicians.
Discussion/conclusion
We present two interesting patient cases who presented with primary lung carcinoma and hypermetabolic foci on FDG PET-CT in the brain that were consistent with epileptic seizures.
The prolonged FDG uptake usually interferes with obtaining ictal PET in contrast to SPECT, in which the tracer Tc-99m-HMPAO can be taken up quickly by the brain and is thus injected right after a seizure takes place [2]. Therefore, an ictal PET is usually an incidental finding. Epileptogenic foci are known to show FDG hypermetabolism in the ictal phase [4]. It is thought that epileptic foci have an increased need for glucose and therefore show as hypermetabolic foci on PET-CT. However, ictal PET data is scarce.Several reports have shown incidental hypermetabolic foci in the brain consistent with epileptic seizures [2,4].
The first case was challenging because the patient presented with widespread metastatic disease, therefore it was reasonable that the hypermetabolic brain lesions were initially interpreted as hypermetabolic metastases. However in 10 to 20% of adults with brain metastases seizures may occur [6]. It was discovered later that the first patient indeed had a seizure justbefore the injection of FDG, thus part of the hypermetabolic areas in the right frontal lobe and the entire hypermetabolic areas contralaterally in the left cerebellar hemisphere turned out to be epileptic foci rather than metastases. The correlation with MRI confirmed this suspicion.
Cerebellar hyperperfusion contralateral to the supratentorial epileptogenic area is often observed on ictal or postictal SPECT scans [7-10]. This phenomenon has been described previously as “crossed cerebellar hyperperfusion”. It may occur because of an increased blood flow in relation to the corticopontocerebellar pathways during epileptic seizures. Since cerebral perfusion and glucose metabolism have been shown to be closely correlated [11], it is expected that a similar pattern could be found as a hypermetabolic area on PET-CT. This has been described in one other previous report in a patient with symptomatic epilepsy without brain metastasis [12]. Our first case also demonstrates this rare phenomenon of crossed cerebellar hypermetabolism caught incidentally on PET-CT.
Foci related to epilepsy described may be visible as hypermetabolic foci on PET-CT up to 48 hours after a seizure [4,13]. However, in the second case the PET-CT was obtained 6 days after the reported absence seizure, which makes it less probable that it would cause hypermetabolic areas. Most likely, the patient had another absence episode perhaps hours before the scan, which hadgone unnoticed by any physicians.
In conclusion, this oncologic case series shows that ictal/ early post-ictal states may be visible on FDG PET-CT making the interpretation of hypermetabolic brain lesions more difficult. A brain MRI can differentiate between metastatic lesions or focal epilepsy by other causes. Clinical information should always be taken into account when interpreting a case with extensive metastatic disease. Moreover, these cases highlight that when hypermetabolic foci in the brain are encountered on PET in patients with a known carcinoma, seizures need to be considered at all times.
References
- Sarikaya I. PET studies in epilepsy. Am J Nucl Med Mol Imaging. 2015; 5: 416–430.
- Horky LL, Treves ST. PET and SPECT in Brain Tumors and Epilepsy. Neurosurg Clin N Am. 2011; 22: 169–184.
- Ponisio MR, Zempel JM, Day BK, Eisenman LN, Miller-Thomas MM, Smyth MD, et al. The Role of SPECT and PET in Epilepsy. Am J Roentgenol. 2021; 216: 759–768.
- Tripathi M, Jaimini A, D’Souza MM, Sharma R, Jain J, et al. Spectrum of brain abnormalities detected on whole body F-18 FDG PET/CT in patients undergoing evaluation for non-CNS malignancies. Indian J Nucl Med IJNM Off J Soc Nucl Med India. 2011; 26: 123–129.
- Knowlton RC. The role of FDG-PET, ictal SPECT, and MEG in the epilepsy surgery evaluation. Epilepsy Behav. 2006; 8: 91–101.
- Lamba N, Catalano PJ, Cagney DN, Haas-Kogan DA, Bubrick EJ, et al. Seizures Among Patients With Brain Metastases. Neurology. 2021; 96: e1237–1250.
- Duncan R, Patterson J, Bone I, Wyper D. REVERSIBLE CEREBELLAR DIASCHISIS IN FOCAL EPILEPSY. The Lancet. 1987; 330: 625–626.
- Park CH, Kim SM, Streletz LJ, Zhang J, Intenzo C, et al. Reverse crossed cerebellar diaschisis in partial complex seizures related to herpes simplex encephalitis. Clin Nucl Med. 1992; 17: 732–735.
- Won JH, Lee JD, Chung TS, Park CY, Lee BI, et al. Increased Contralateral Cerebellar Uptake of Technetium-99m-HMPAO on letal Brain SPECT.
- Umemura A, Suzuka T. Crossed Cerebellar Hyperperfusion in Symptomatic Epilepsy. Neurol Med Chir (Tokyo). 2000; 40: 65–68.
- Franck G, Sadzot B, Salmon E, Depresseux JC, Grisar T, et al. Regional cerebral blood flow and metabolic rates in human focal epilepsy and status epilepticus. Adv Neurol. 1986; 44: 935–948.
- Kawai N, Kawanishi M, Tamiya T, Nagao S. Crossed cerebellar glucose hypermetabolism demonstrated using PET in symptom atic epilepsy--case report. Ann Nucl Med. 2005; 19: 231–234.
- Leiderman DB, Albert P, Balish M, Bromfield E, Theodore WH, et al. The dynamics of metabolic change following seizures as measured by positron emission tomography with fludeoxyglucose F 18. Arch Neurol. 1994; 51: 932–936.