
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Large retrosternal non-hodgkin’s lymphoma presenting
with recurrent syncope episodes and chest
asymmetry: A case report
Bashar Wannous1*; Nour Sadran2; Aram Abbas3; Mohammad Awwad1; Bayan Alhasan4; Hosam Mansour4; Mohammad Hasan1
1Faculty of Medicine, Hama University, Hama, Syria.
2Faculty of Medicine, Aleppo University, Aleppo, Syria.
3Al Mouwasat University Hospital, Damascus, Syria.
4Masyaf National Hospital, Hama, Syria.
*Corresponding Author : Bashar Wannous
Faculty of Medicine, Hama University, Hama, Syria.
Email: Basharwanos20@gmail.com
Received : Mar 25, 2023
Accepted : Apr 17, 2023
Published : Apr 24, 2023
Archived : www.jcimcr.org
Copyright : © Wannous B (2023).
Abstract
In this case we report a 42-year-old woman who presented to Syrian Heart Lung Center (SHLC) with recurrent syncope attacks, general fatigue and weight loss. During the diagnostic approach, many investigations were performed including laboratory analysis, ECG, Echocardiography, Computed Tomography (CT), and biopsies. However, immunostaining was the decisive investigation. The patient was finally diagnosed with large B cell lymphoma, which is a type of Non- Hodgkin’s lymphoma (NHL). NHL is a type of malignancies that arise from lymphoid tissue, basically the lymph nodes. Patients with NHL usually present with painless lymphadenopathy causing multiple symptoms, including B symptoms (fever, weight loss and night sweats). However, our patient’s main complaint was recurrent syncope attacks which is considered an unusual manifestation in the case of NHL. These syncope episodes were most likely due to the compressive effects on the vascular system that resulted in less venous return to the heart which ended in a low cardiac output. The patient was treated with R-CHOP regimen and showed improvement. The syncope attacks dissolved and the jugular congestion was resolved.
Keywords: Non Hodgkin’s lymphoma; Syncope attacks; Pleural effusion; Retrosternal extension.
Citation: Wannous B, Sadran N, Abbas A, Awwad M, Alhasan B. Large retrosternal non-hodgkin’s lymphoma presenting with recurrent syncope episodes and chest asymmetry: A case report. J Clin Images Med Case Rep. 2023; 4(4): 2383.
Introduction
A tumor is an abnormal proliferation caused by uncontrolled cellular divisions or when there are defects in apoptosis and the cell cycle [1]. The abnormal proliferation of lymphoid tissue that affects either lymphoid cells or their precursors is known as lymphoma [2]. Lymphoma is divided into Hodgkin’s lymphoma which constitutes nearly 10%, and Non-Hodgkin’s Lymphoma (NHL) which constitutes the remaining 90% [3]. NHL could be hard to be diagnosed because it has many different histological and clinical features (To Be Found). Painless lymphadenopathy persisting for more than 2 weeks, is the typical presentation for about two thirds of NHL cases. Other patients could present with other signs and symptoms such as mediastinal lymphadenopathy, pleural effusion, diffuse hepatosplenomegaly, fever of unknown origin, unexplained weight loss, persistent cough, chest discomfort, anorexia, nausea, vomiting and abdominal pain [4]. In this article, we highlight an unusual manifestation of NHL in a 42-year-old Syrian female that presented to Syrian heart lung center (SHLC) complaining of recurrent syncope attacks and chest tightness.
Case presentation
Patient information and clinical findings
A 42-year-old Syrian female presented to the Syrian heart lung center (SHLC) with general fatigue and appetite loss, her weight six months prior to the visit was 69 Kg, at the visit she weighed 40 kg. She did not experience any chest pain but mentioned recurrent syncope during the last month. In the previous two weeks, the patient suffered from chest tightness with a productive cough, increasing on lying position. Clinical examination.
Vital signs
Blood pressure (BP) 100/50 mmHg, body temperature 37.6oc (orally), respiratory rate (RR) 24/min, heart rate (HR) 100 beat/min. The patient looked pale and dyspneic. During inspection, we noticed skin rash on the left hand, associated with itching (figure 1), fixed bilateral external jugular venous distention, crusted skin pustules (figure 2), and bulging in the left subclavian region causing chest asymmetry (retrosternally) (figure 3). On percussion we noticed dullness on the left side of the chest. On auscultation the left side exhibited diminished lung sounds. However, the breath sounds were normal on the right side except muffled breath sounds on the basal stripe.
Complementary investigations
We ordered complete blood test, results are shown in table 1. Chest X-Ray (CXR) showed severe left-sided pleural effusion causing mild tracheal deviation (Figure 4). Drainage and examination of the pleural effusion (about 2 liters) showed yellow turbid fluid. Microscopic examination showed RBCs: 302 cell/mm3, white blood cells (WBCs): 230 cell/mm3 (neutrophils 70%, lymphocytes 30%). The chemical examination showed elevated glucose (96 mg/dl), protein (5.6 g/dl), and LDH (762 U/L). Pleural fluid cytology examination showed a pattern of benign hemorrhagic findings of reactive inflammatory type and didn’t show any evidence of abnormal cells. Pleural fluid was negative for TB.
We did Electrocardiography (Figure 5). It showed sinus tachycardia, mild abnormal intraventricular conduction disorder, tall R waves on left leads and normal cardiac axis. The systolic function, and diastolic function were normal. Right heart chamber sizes were normal too. Valves examination showed trace regurgitation in the mitral valve, the aortic valve had tri-cusps with normal gradient, the pulmonary valve was normal, and the tricuspid valve showed mild regurgitation with no significant gradient change.
Chest CT (without contrast) was performed after the drainage of pleural fluid from the left side (Figure 6). It revealed moderate bilateral pleural effusion, more in the right side. It also showed lymphadenopathy (LAP) in the neck base and the retrosternal space in the upper-anterior mediastinum, attached to the lower lobe of the thyroid gland, causing deviation of the trachea to the right side. We also found a compressive effect of the LAP on the neck vessels, and infiltrates in the left lung probably due to atypical pneumonia. Then we performed CT with contrast (Figure 7).
After few days, we performed lower cervical lymph node excisional biopsy, the lymph node measured 2 x 1 cm diameter and the microscopic examination reveal lymph node tissue showing a diffuse polymorphous lymphoid hyperplasia with distention and prominence of the lymphatic sinusoids, and benign lymphoid follicles, and a mixed population of lymphocytes in different stage of differentiation with histiocytes and plasma cells and there was no histologic evidence of granulomas or tuberculosis (TB). It showed no cellular atypia or malignancy. The result was benign lymph node reactive hyperplasia. We performed another excisional biopsy for 4 lymph nodes from the side of the left internal carotid artery, the largest measured 2.5 x 1.5 cm diameter. The microscopic examination of serial sections revealed effacement of the follicular architecture of the lymph node, with diffuse infiltration by transformed lymphoid cells “immunoblasts” and Hodgkin’s cells and histiocytes. The result confirmed Hodgkin lymphoma, lymphocyte depleted type. Immunostaining of the biopsies showed diffuse infiltration of large B cell non-Hodgkin lymphoma, accompanied with extranodal infiltrates, Positive staining for CD20, Negative for CD3, CD30 & CD15, indicating large B cell lymphoma. We did an 8 mm bone marrow biopsy and it showed no sign of any infiltrative lesion. The cellularity was proportional to the age of the patient and the three bloodlines were present with maturity.




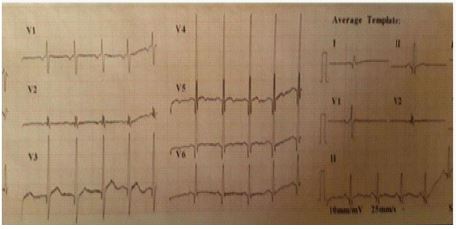

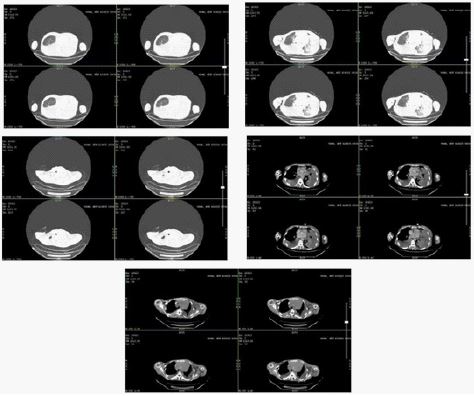
Table 1: Complete blood tests of the patient
| Red blood cells (RBCs) | 4 x 106mm3 |
| MHCH | 33.33% |
| MCV | 60.00 FL |
| MCH | 20 Pg |
| Hemoglobin | IP/88 |
| Hematocrit | 24.00% |
| White blood cells (WBCs) | 11500/mm3 |
| Neutrophils | 73% |
| Lymphocytes | 25% |
| Monocytes | 1% |
| Platelets | 215 x 1000/mm3 |
| ESR | First hour: 60 mm Second hour: 110 mm |
| CRP | 135 mg/1 |
| Total proteins | 5.7 g/d1 |
| Albumin | IP/87 |
| Globulin | 3.7 g/d1 |
| Albumin/Globulin | 0.54 |
| Creatinine | 0.56 mg/dl |
Treatment
The patient was given antibiotics (Moxifloxacin 400 mg 1 tablet per day for 1 week, and Ceftazidime 1 g intravenously 3 vial per day for 4 days) to treat the suspected coexisting pneumonia, and Prednisolone 20 mg 2 tablets per day for 1 week while waiting for the biopsy result, which caused significant clinical relief. Then the patient started the chemotherapy (Vinblastine 3.7 mg/m2 intravenously, and Doxorubicin 6 mg/m2 intravenously) while waiting for the immunostaining results. After we received the immunostaining results, we started the specific treatment for NHL, which is R-CHOP (Rituximab 375 mg/m2, Cyclophosphamide intravenously 750 mg/m2,Doxorubicin 50 mg/m2, Vincristine 1.4 mg/m2, and Prednisolone orally 40 mg/m2). The patient also started taking Allopurinol 300 mg per day orally for controlling uric acid levels, and Rivaroxaban 10 mg 1 tablet per day orally for preventing clots and strokes. After this management, the patient did not have any syncope episode, cough, or chest tightness. The jugular venous congestion was also resolved. Now, we continue to give the patient the required chemotherapy, with continuous surveillance and follow-up of the patient’s status.
Discussion
The most common clinical presentation of mediastinal NHL is a fast-growing mass in the anterior mediastinum, which usually causes respiratory symptoms, and B symptoms (fever, night sweats, and weight loss) [5]. However, our patient’s manifestations were different representing mainly by recurrent syncope attacks and weight loss. Because syncope reflects underlying disease and is not classified as a disease itself [6]. A thorough physical examination and investigations were made in order to determine the cause. During the diagnostic approach, ECG should be done in all patients with syncope presentation [6]. in order to exclude any causing underlying cardiac lesions (Our ECG findings were mentioned in the case presentation). In addition, CT is the first-line examination method that can detect lymph node enlargement, Imaging findings include unilateral diaphragm elevation, pleural effusion and pericardial effusion [7]. The patient in our case had pleural effusion which needed pleurocentesis for both diagnosis and relieving the patient symptoms. When there are nearly 75% of the blood inside the veins, any disturbance in the intravenous return may cause a reduced cardiac output [6]. This supports one of many mechanisms in case of syncope. The suggested pathophysiology is represented by reduced venous return to the heart due to compressive effects of the conglomerated cervical and retrosternal lymph nodes, and loss of preload volume in the third chamber (pleural cavity), in addition to suspected autonomic effects on vascular system. Starting the diagnosis of mediastinal NHL is a challenge for healthcare professionals, as It may be hard to differentiate from mediastinal nodular sclerosis Hodgkin’s lymphoma due to the overlap in the histological findings [8-10].
Even though our patient is a middle-aged woman, Mediastinal NHL usually occurs in young people [11]. Currently, our patient is being managed with R-CHOP regimen as it is considered the first-line treatment for the large B-cell non-Hodgkin’s lymphoma according to the National Comprehensive Cancer Network (NCCN) guidelines [12].
Conclusion
As it turned out, the diagnosis of mediastinal tumors is generally difficult, and the various histological and clinical features of mediastinal NHL make the diagnosis more complicated. In this case, we are highlighting the necessity of taking NHL into consideration while dealing with a patient presenting with mediastinal mass with recurrent syncope attacks. However, in order to avoid misdiagnosis, wide investigations and histological studies should be performed and immunohistochemical tests should be completed.
References
- Patel A. Benign vs Malignant Tumors. JAMA Oncology. 2020; 6(9): 1488.
- Lu P. Staging and Classification of Lymphoma. Seminars in Nuclear Medicine. 2005; 35(3): 160-164.
- Shankland KR, JO Armitage, BW Hancock. Non-Hodgkin lymphoma. The Lancet. 2012; 380(9844): 848-857.
- Mawardi H, C Cutler, N. Treister. Medical management update: Non-Hodgkin lymphoma. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology. 2009; 107(1): e19-e33.
- Martelli M, et al. Primary mediastinal large B-cell lymphoma. Critical Reviews in Oncology/Hematology. 2017; 113: 318-327.
- Grossman SA, M Badireddy. Syncope, in StatPearls. 2023, StatPearls Publishing Copyright © 2023, StatPearls Publishing LLC Treasure Island (FL).
- Pfau D, et al. Primary Mediastinal Large B-Cell Lymphoma: A Review for Radiologists. American Journal of Roentgenology. 2019; 213(5): W194-W210.
- Jaffe, E.S., The 2008 WHO classification of lymphomas: implications for clinical practice and translational research. Hematology, 2009. 2009(1): p. 523-531.
- Rosenwald A, et al. Molecular Diagnosis of Primary Mediastinal B Cell Lymphoma Identifies a Clinically Favorable Subgroup of Diffuse Large B Cell Lymphoma Related to Hodgkin Lymphoma. Journal of Experimental Medicine. 2003; 198(6): 851-862.
- Savage KJ. The molecular signature of mediastinal large B-cell lymphoma differs from that of other diffuse large B-cell lymphomas and shares features with classical Hodgkin lymphoma. Blood. 2003; 102(12): 3871-3879.
- Wang Y, et al. Case Report: Primary Mediastinal Large B-Cell Lymphoma Invasion of Extranodal Thyroid Tissue Mimicking Tuberculosis and Confounded by Similar Ultrasonic Appearance. Frontiers in Oncology. 2022; 12.
- Yu, Y., et al., Primary mediastinal large B cell lymphoma. Thoracic Cancer. 2021; 12(21): 2831-2837.