
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Series - Open Access, Volume 4
Post COVID vaccination combined central and peripheral
demyelination: Case series and review
Samhita Panda1*; Apoorv Patel1; Monalisa Vegda1; Sarbesh Tiwari2
1Departments of Neurology, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
2Diagnostic and Interventional Radiology, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
*Corresponding Author : Samhita Panda
Additional Professor and Head, Department of Neurology, All India Institute of Medical Sciences, Jodhpur, Rajasthan, India.
Phone: 91-0-9810838268 (Office);
Email: samhitapanda@yahoo.com
ORCID id: 0000-0002-8162-3060.
Received : Mar 23, 2023
Accepted : Apr 18, 2023
Published : Apr 25, 2023
Archived : www.jcimcr.org
Copyright : © Panda S (2023).
Abstract
Combined Central and Peripheral Demyelination (CCPD) is a rare neurological disorder in which demyelination occurs in the central as well as peripheral nervous systems, either sequentially or simultaneously. While neurological complications have been reported anecdotally after COVID vaccination, this report highlights the rare occurrence of CCPD in three patients during this period with stress on variations in their presentation, course of progression and response to treatment and outcome. The existing literature has also been reviewed to improve our understanding of this uncommon disorder.
Keywords: Combined central and peripheral demyelination; Demyelinating neuropathy; Myelitis; Multiple sclerosis; Vaccination; COVID-19.
Citation: Panda S, Patel A, Vegda M, Tiwari S. Post COVID vaccination combined central and peripheral demyelination: Case series and review. J Clin Images Med Case Rep. 2023; 4(4): 2385.
Introduction
Acquired demyelinating disorders of Central Nervous System (CNS) and Peripheral Nervous System (PNS) are infrequent. In comparison, Combined Central and Peripheral Demyelination (CCPD) is an even rarer clinical disorder. CCPD encompasses demyelination in both CNS and PNS, either sequentially or simultaneously [1,2]. CNS involvement may be localised to optic nerves, grey matter and/or extensive spinal cord involvement and may mimic MS while PNS involvement occurs mainly as CIDP-like disease with primary triggers of infections and vaccination [1-3]. During the COVID-19 pandemic, demyelination was observed in PNS and CNS in relation to other neurological manifestations. While emergency approval of vaccines developed from different countries was done to curb the impact of COVID, post-vaccination neurological complications have been reported from around the world. This report highlights the rare occurrence of CCPD in 3 patients during this period and reviews existing literature to understand the variations.
Case 1
A 50-year-old lady, hypothyroid on treatment, presented with facial weakness and perioral numbness for 10 days. Two days later she developed bilateral lower limb weakness andvomiting with sequential weakness of left upper limb and then both upper limbs. She had received COVID vaccine (AstraZeneca- ChAdOx1-S) 20 days prior to symptom onset immediately following which she had fever and fatigue.
Examination revealed bilateral lower motor neuron 7th nerve palsy. There was generalized hypotonia and quadriparesis- lower more than upper limbs, proximal more than distal with neck and truncal weakness and generalized areflexia. Plantar reflexes were flexor with no sensory or cerebellar signs. Single breath count was less than 15/minute.
Nerve Conduction Studies (NCS) showed generalised symmetrical predominantly demyelinating sensorimotor polyneuropathy (supplementary material Table 1). Cerebrospinal Fluid (CSF) analysis was paucicellular with elevated protein (215 mg/dL). Screening for HIV, HBsAG, HCV, Lymes and Scrub typhus and inflammatory conditions including connective tissue disorders and sarcoidosis was negative. COVID serology was positive for IgG for SARS-CoV-2 by ELISA. Serology was negative for ganglioside autoantibodies (GM1, GM2, GM3, GD1a, GD1b, GT1b and GQ1b by Immunedot blot method).
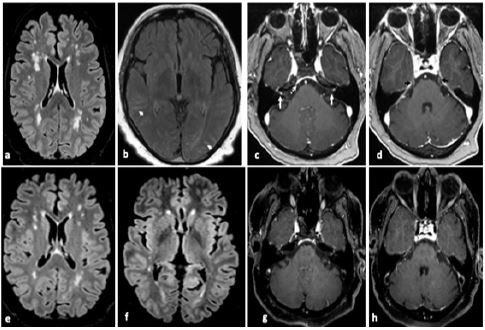
Considering Acute Inflammatory Demyelinating Polyneuropathy (AIDP), Intravenous Immunoglobulin (IVIG) was given without significant improvement. At this juncture, contrast-enhanced MRI brain showed punctate T2 hyperintense and T1 hypointense lesions in subcortical, periventricular and deep white matter with leptomeningeal and cranial nerve enhancement (Figure 1a-d). Considering CCPD, pulse Intra Venous Methyl Prednisolone (IVMP) followed by oral steroids was given with gradual improvement. At 18-month follow-up, MRS was 0 with significant resolution of MRI abnormalities.
Case 2
This 40-year-old farmer developed upper back pain 4 days prior to admission with rapid progression to lower backache, band-like sensation over abdomen and radiation to both lower limbs. Next day he noticed bilateral lower limb weakness and paraesthesias that progressed to upper limbs and trunk. Perioral paresthesia, occasional diplopia, choking and change in voice was noted along with generalized pain, constipation and straining on micturition. He had received COVID-19 vaccination (Astra Zeneca- ChAdOx1-S) 15 days prior to symptom onset.
On examination, he had bilateral 6th and lower motor neuron 7th cranial nerve palsy, quadriparesis and generalized areflexia. Plantar responses were mute and abdominal reflexes absent. There was reduction of touch, pain and temperature below C7 level (50%). Single breath count was 50. He was able to walk with support of one person, Hughes GBS Disability scale- 3 and MRC Disability Scale- 5.
A provisional diagnosis of GBS was made with red flag signs (bowel, bladder involvement and sensory level). All haematological and biochemical tests were unremarkable. NCS suggested AIDP (supplementary material Table 1). CSF showed protein- 310 mg/dL, sugar- 87 mg/dL and 35 cells/dL, predominantly lymphomononuclear. Serology for ganglioside autoantibodies was negative. Serum was positive for IgG against SARS-CoV-2. MRI spine showed thickening and enhancement of conus, cauda equina nerve roots and filum terminale (Figure 2a-c).

Pulse IVMP was given empirically due to initial financial constraints with some improvement. Nadir was reached after 8 days with Hughes scale of 4 and MRC disability scale of 6. Subsequently, after waiver of charges, 5 cycles of Plasma Exchange (PLEX) were done with improvement to residual grip weakness and mild improvement in lower limbs.
However, he had recurrence of limb weakness after 15 days progressing to suspended sensory loss over neck and trunk with bilateral 5th, 7th, 9th and 10th cranial nerves without bowel and bladder involvement. There was hypertonia in both upper limbs. Cremastric, abdominal reflexes and plantar responses were absent. Touch, pain and temperature reduction of 50% was seenfrom C2 to L3 level. Propioception was absent up to ankle and wrist joints. Single breath count had dropped to 23. Possibility of treatment related fluctuations versus additional longitudinal myelitis was kept.
NCS also showed worsening with additional facial nerve demyelination. CSF was paucicellular with protein- 219 mg/dL. Contrast enhanced MRI brain was normal and MRI spine showed no evidence of myelitis. However, Visual Evoked Potentials (VEP) showed bilateral P100 latency prolongation leading to diagnosis of MRI negative myelitis. As there was only partial improvement with Intravenous Immunoglobulin (IVIg), IVMP was given again.
He improved symptomatically over next 9 months. However, NCS continued to worsen further in the initial 5 months progressing to unrecordable sensorimotor potentials in lower limbs with subsequent recovery (supplementary material Table 1). Azathioprine was continued and at 18 month follow up he had no neurological deficit except occasional sensation of lower limb numbness, improvement in NCS and complete resolution of cauda equina nerve root enhancement on MRI.
Case 3
A 56-year-old gentleman presented with headache and recurrent vomiting for 2 days followed by numbness of right half of face, right lower limb imbalance and clumsiness of ipsilateral hand. There was no preceding fever, cough, sore throat. He had received second dose of COVID vaccine (AstraZeneca- ChAdOx1-S) 15 days prior to onset. In March 2020 he had developed flaccid areflexic quadriparesis diagnosed as GBS (AIDP variant) around the beginning of COVID-19 pandemic in India (supplementary material Table 1). However, COVID RT-PCR test kits were not yet available then. Ganglioside panel was positive for IgG antibodies to GD1b and GM1 and he had been treated with PLEX with complete improvement.
Now 18 months later, examination revealed decreased touch (80%) on right half of face, right lower limb hypotonia and ataxic gait. Plantar responses were flexor. CSF showed protein 137 mg/dL, sugar 66 mg/dL and 30 lymphomononuclear cells/cumm. MRI brain showed right middle cerebellar peduncle T2 hyperintensity suggesting demyelination (Figure 1e-h). COVID RT-PCR was negative though serum was positive for IgG against SARS-CoV-2. Work up for stroke, secondary demyelination and serum protein electrophoresis was negative. CSF for oligoclonal bands and NMO-MOG was negative. NCS showed motor predominant axonal neuropathy (recovering from previous insult). VEP, SSEP andwhole-body PET was normal.
Pulse IVMP followed by oral steroids was given. He improved symptomatically over next 7 months even though the NCS continued to worsen over the initial 6 months with drop in CMAP amplitudes in upper limbs. Azathioprine was added and at 1 year follow up he had no neurological deficit, complete radiological resolution and generalized improvement in CMAP amplitudes.
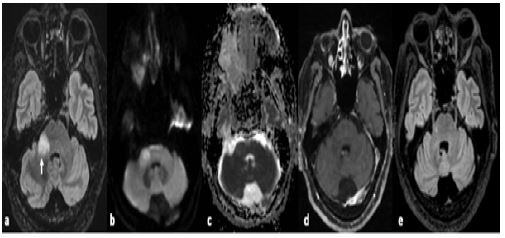
Table 1: Review of clinical and laboratory features of CCPD cases in literature.
| Author | Year of publication | Number of cases | Etiological agent | Clinical features | Investigations | Treatment received | Outcome |
|---|---|---|---|---|---|---|---|
| Cortese A, J Neurol Sci [1] | 2016 | 31 (majority male; median -57 years) | 65%- infection and vaccination | Myeloradiculoneuropathy, encephalopathy, cranial neuropathy, length-dependent peripheral neuropathy, or pseudo-Guillain-Barré syndrome | Demyelinating polyneuropathy- 74%, demyelinating lesions on brain MRI- 73%; MRI spine- T2 lesions in 80% | Steroids, IVIG, or PLEX | Monophasic in one-third; 21 had relapse; subacute to chronic progression; 71% who were left significantly disabled |
| Ogata H, JNNP [2] | 2016 | 40 (29 female) | 4- infections, 1- vaccination, rest- no trigger | Sensorimotor involvement of limbs, gait disturbance | Anti-NF155 (45.5%), OCB (7.4%), abnormal VEP (71.4%) | IVIg (66%), PLEX (87.5%), steroids (83.3%) | Improvement on steroids |
| Hou X, MS J [3] | 2021 | 31 | Data not available | Motor (83%), sphincter (58%) involvement, hyporeflexia (63%) | Anti-NF155 (20%), anti-AQP4 (21%), anti-MAG (10%), abnormal VEP (33%) | IVIg (37.5%), rituximab (100%), steroids (72.2%) | mRS 4 in 37% |
| Katchanov J, JNNP [4] | 2004 | 1 (32/F) | Fever-? etiology | Flaccid quadriparesis, bladder involvement, nystagmus | CSF- pleocytosis (34/mm3) Protein-132 mg/dL; no OCB, Ganglioside Ab- positive for asialo-GM1, GM1 and GQ1b; MRI spine- extensive cervicothoracic myelopathy; MR brain-multiple demyelinating lesions in frontoparietal gray and white matter; NCS- severe symmetrical demyelinating neuropathy | IVIg pulse followed by PLEX after failure of IVMP | Residual ataxia at 1 year |
| Hernández RC, Neurologia [5] | 2017 | 1 (58/F) | No trigger | Multifocal sensorimotor involvement | NCS- motor asymmetric polyneuropathy; MR brain- normal; MRI spine- T2 hyperintensity in spine; VEP-abnormal | IVIg | Improved |
| Nouha H, Iran J Neurol [6] | 2019 | 1 (20/M) | No trigger | Cerebellar ataxia; later flaccid quadriparesis | MRI brain- multiple demyelination; MRI spine- multilevel eccentric signal changes; VEP- prolonged; NCS-demyelinating polyneuropathy | B-interferon; IVMP- no improvement; later PLEX | Some improvement |
| Harada M, Neurology [7] | 2019 | 1 (60/F) | No trigger | Constipation, progressive paraparesis, areflexia | MRI brain- demyelination in medulla; MRI spine- myelitis; NCS- multifocal demyelinating polyneuropathy; OCB-positive; Ab to lactosylceramide-positive | PLEX + steroids | Relapsed with steroid responsiveness |
| Alshamrani F, Frontiers in Neurology [8] | 2021 | 2021 | No trigger | Ataxia, ophthalmoplegia, and areflexia like MFS, constipation | MRI spine- cervicothoracic demyelination; MR brain- multiple demyelinating lesions; CSF OCB-positive; proteins raised; NCS- normal; Anti-GQ1b positive | IVMP- worsening; then PLEX | Improved; mild ataxia at 7 months |
| Lambrianides S, The Neurologist [9] | 2021 | 1 (30/M) | No trigger; Father had MS | Numbness, gait impairment | Anti NF 155-positive | No response to IVIg; then rituximab given | Symptoms stabilized |
| Makkawi S, Cureus [10] | 2021 | 1 (29/M) | No trigger | Progressive lower and upper limb weakness; facial and arm tremor; urinary hesitancy | MRI brain- multiple demyelinating plaques; MRI spine- multilevel eccentric signal changes; NCS-demyelinating polyneuropathy; VEP- prolonged | PLEX followed by IVMP; then IVIg, Azathioprine, rituximab | Recurrent flareups on steroid taper, stabilized with rituximab |
| Coehlo P, J Neurol [11] | 2022 | 1 (48/M) | COVID vaccination (AstraZeneca- ChAdOx1)-started after 1st dose, progressed after 2nd dose | Anosmia, ageusia, Myelopathy, ataxia | MRI brain- normal; MRI spine- myelitis; NCS-sensorimotor demyelinating polyneuropathy | IVMP pulse followed by oral steroids | Improvement at 8 months |
| Matteo E, Can J Neurol Sci [12] | 2022 | 1 (52/M) | COVID vaccination (AstraZeneca- ChAdOx1)-started after 1st dose | First episode-Multiple cranial nerve palsy, sensory ataxia Second episode- after 15 days, bilateral optic neuritis |
MRI brain- normal; MRI spine-contrastenhancement of cauda equina roots; NCS- distal predominant demyelinating polyradiculoneuropathy Repeat MRI brain- contrast-enhancing multifocal bilateral demyelinating lesions;Serum positive for anti-NF155 IgG autoantibodies |
IVIG- partial response with relapse IVMP pulse and oral steroids |
Completely recovered after 2 months |
| Al Kolfat F, Neuroimmunol Rep [13] | 2022 | 1 (23/M) | ChAdOx1 nCoV-19 vaccine- started after 1st dose | Areflexic quadriparesis; sensory level till neck | MRI brain and spine- nonspecific central demyelination; NCS-sensorimotor demyelinating polyneuropathy; No OCB | Steroids; then PLEX | Complete improvement |
Discussion
Initially described by paediatricians as encephalo-myelo-radiculo-neuropathy, the term CCPD was coined by Katchanov for a rare neurological disorder with heterogeneous manifestations along multiple locations in the neuraxis [4]. CCPD manifests as encephalopathy, cranial neuropathy, optic neuritis, myeloradiculoneuropathy, peripheral neuropathy and GBS-like syndrome [1-3]. Chronologically, CNS involvement may precede, succeed or occur alongside PNS manifestations either clinically or on radiological or electrophysiological investigations. Likewise their presentation maybe acute, relapsing–remitting and chronic. These dichotomies of CCPD are exemplified in the present case series of post COVID vaccination CCPD. Case 1 had clinical PNS manifestation while CNS involvement was detected after investigations. Case 2 was symptomatic for both CNS and PNS involvement with fluctuations though radiologically negative for CNS involvement. On the other hand, case 3 had sequential involvement of PNS followed by CNS after 18 months.
Most cases of CCPD are single reports or series, the largest comprising of 40 patients, exemplifying its rarity. Table 1 shows the clinical characteristics of patients reported in world literature [1-13]. Infections constitute majority of known triggers of CCPD, which rarely follows influenza and pneumococal vaccination. In most cases no obvious trigger was found. Contrary to literature, occasional CCPD has been noted after COVID vaccination [11-13]. This intuitively outlines the dysimmune interactions of vaccination. The mass COVID vaccination has proved partly instrumental in subverting serious COVID infections using number of technologically different vaccines. However, occurrence of adverse events following immunization cannot be denied. All 6 patients with CCPD developed symptoms in close temporal relation to vaccination by AstraZeneca-ChAdOx1. It may be speculated that the live attenuated spike protein vaccine may cause CCPD either directly by binding to sialic acid-containing glycoproteins and gangliosides or via adenovirus vector. Only in Case 3, a case of molecular or antigenic cross reactivity between putative COVID infection in the first wave and later vaccination is a possibility.
Pathophysiologically, it is unclear whether CCPD results from a cross-reactive immune response to antigen in either PNS or CNS or presence of same antigenic target in both. Kawamura et al demonstrated elevation of antibodies against Neurofascin (NF), a transmembrane adhesion molecule of L1 subgroup expressed at nodes of Ranvier and paranodes in both CNS and PNS in 86% CCPD patients [14]. In addition to NF-155, antibodies against NF-186, galactocerebroside and lactosylceramide have been noted [2,3,7,9]. Amongst post-COVID vaccine-related CCPD, only Matteo et al reported anti-NF155 auto antibodies [12]. However, there are also reports of CCPD without positive NF-155 antibodies, such as our cases, highlighting the complexity of finding potential epitopes and effect of ethnicity.
Clinical diagnosis of CCPD is usually uncertain initially as patients present as GBS, CIDP or MS and are treated accordingly while either imaging or subsequent relapse involving different sites suggests CCPD (Table 2) [1,5,6,8]. Hence, it is debatable whether CCPD is a single condition due to common immunopathogenic mechanism or two coincidental demyelinating disorders. Importantly, application of individual diagnostic criteria does not cover the entire spectrum seen in a patient. Our cases highlight red flags for pure PNS involvement like sensory level and sphincter involvement that may suggest added CNS insult [8,10,13]. Also, sequential involvement may occur as in Case 3 [6,12]. Further adding to the complexity is the lack of consistency of biochemical/ immunological abnormalities seen in the aforementioned demyelinating disorders.
The progression of CCPD has varied across studies [1,2]. In one of the biggest cohorts, 65% had no or mild disability after the acute phase, in contrast to Cortese et al who demonstrated poor outcome in 71% with progressive cumulative neurological impairment despite immunosuppression [1,2]. Invariably, initial site of involvement influences the first treatment choice, as those with early PNS involvement might receive IVIg/plasmapheresis rather than steroids [4,6,7]. Patients with simultaneous onset of peripheral and central disease are more likely to have a monophasic course and better treatment response, as in our case [2]. Cortese et al showed that relapse-remitting and chronic progressive subgroups had poor treatment response with disease recurrence [1]. IVIg and PLEX are also treatment options in steroid failure in CCPD [7]. Kawamura suggested a better response to IVIG or PLEX in patients positive for anti-NF antibodies. However, we noted good response to IVMP in COVID vaccination related CCPD, failing which PLEX was effective [11-13]. There are also reports of halting of disease progression with rituximab [9,10].
Conclusion
While COVID vaccines are undoubtably helped reduce infection severity and need for hospitalization, we have been intermittently reminded of their adverse effects. CCPD is a rare autoimmune manifestation that may occur in close temporal association with COVID vaccine though a true causal link may be difficult to prove. The stress should be on early recognition and longer treatment protocol in view of tendency to progress or relapse.
Declarations
Acknowledgements: The authors would like to thank the department of Transfusion Medicine of All India Institute of Medical Sciences, Jodhpur, for the diagnostic and management support provided in some of the patients in this study.
Author contributions: SP- 1) conception and design of the study,
2) acquisition and analysis of data,
3) drafting a significant portion of the manuscript or figures.
AP- 1) conception and design of the study,
2) acquisition and analysis of data
MV- 1) acquisition and analysis of data,
2) drafting a significant portion of the manuscript or figures.
ST- 1) acquisition and analysis of data,
2) drafting a significant portion of the manuscript or figures.
Potential conflicts of interest: Nil.
Conflict of interest: Nil.
Financial support: Nil.
References
- Cortese A, Franciotta D, Alfonsi E, et al. Combined central and peripheral demyelination: Clinical features, diagnostic findings, and treatment. J Neurol Sci. 2016; 363: 182–87.
- Ogata H, Matsuse D, Yamasaki R, et al. A nationwide survey of combinedcentral and peripheral demyelination in Japan. J Neurol Neurosurg Psychiatry. 2016; 87: 29-36.
- Hou X, Liang Yan, Cui P, Hao J. The clinical features of combined central and peripheral demyelination and antibodies against the node of Ranvier. Mult Scl J. 2021; 28: https://doi.org/10.1177/13524585211028126.
- Katchanov J, Lu¨nemann JD, Masuhr F, Becker D, Ahmadi M, et al. Acute combined central and peripheral inflammatory demyelination. J Neurol Neurosurg Psych. 2005; 75: 1784-1786.
- Hernández RC, Mañas RG, Molinero JG. Combined central and peripheral demyelination: A case description. Neurologia. 2017; 32: 547-550.
- Nouha H, Olfa H, Nouha F, et al. Combined central and peripheral demyelination: A case report and literature review. Iran J Neurol. 2019; 18: 35-37.
- Harada M, Miura S, Kida H, et al. Reversible Conduction Failure in Anti lactosylceramide-antibody-positive Combined Central and Peripheral Demyelination. Front Neurol. 2019; 10: 600.
- Alshamrani F, Alyami R, Alghanimi I, et al. A New Report of Combined Central and Peripheral Demyelination: A Case Report. Front Neurol. 2021.
- Lambrianides S, Kinnis E, Cleanthous M, et al. A Case of Combined Central and Peripheral Demyelination Associated With Antineurofascin 155 Antibodies and Paternal History of Multiple Sclerosis. Neurologist. 2021; 26: 156-159.
- Makkawi S, Yonbawi F, Qari Y, Aljinaid M. Combined Central and Peripheral Demyelinating Disease With Good Response to B-Cell Depleting Therapy. Cureus.
- Coelho P, Paula A, Martins IV, de Campos CF, Ferreira J, et al. Combined central and peripheral demyelination after COVID‑19 vaccination. J Neurol. 2022; 269: 4618-4622. https://doi.org/10.1007/s00415-022-11188-7.
- Matteo E, Romoli M, Calabrò C, Piccolo L, Lazzarotto T, et al. Combined Central and Peripheral Demyelination withAnti-Neurofascin155 IgG Following COVID-19 Vaccination. Can J Neurol Sci. 2022; 1-3.
- Al Kolfat F, Elfatatry A, Mekky J, Aly AS. Combined peripheral and central nervous system demyelination post-COVID-19 vaccination: A case report. Neuroimmunol Rep. 2022; 2: 100057. https://doi.org/10.1016/j.nerep.2022.100057.
- Kawamura N, Yamasaki R, Yonekawa T, Matsushita T, Kusunoki S, et al. Anti-neurofascin antibody in patients with combined central andperipheral demyelination. Neurology. 2013; 81: 714-722.