
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Posterior urethroplasty and recto-urethral fistula repair by
bulbospongiosus muscle flap: A new surgical technique
Alimohammad Mirjalili1; Seyed Masoud Hosseini2; Ehsan Shojaeefar3; Saeid Abouei4*
1Reconstructive Urologist, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
2Department of General Surgery, Shahid Sadoughi University of Medical Sciences, Yazd, Iran.
3Immunology Board for Transplantation and Advanced Cellular Therapeutics (ImmunoTACT), Universal Scientific and Education Network (USERN), Tehran, Iran.
4Medical doctor, Andrology Research Center, Yazd Reproductive Science Institute, ShahidSadeghi University of Medical Sciences, Yazd, Iran.
*Corresponding Author : Saeid Abouei
Medical Doctor, Andrology Research Center, Yazd Reproductive Science Institute, Shahid Sadeghi University of Medical Sciences, Yazd, Iran.
Email: saeidabouei74@gmail.com
Received : Mar 20, 2023
Accepted : Apr 20, 2023
Published : Apr 27, 2023
Archived : www.jcimcr.org
Copyright : © Abouei S (2023).
Abstract
Introduction: Recto-Urethral Fistula (RUF) is a relatively uncommon surgical condition requiring complex and precise surgery that is often challenging for surgeons. There is no firm consensus on the surgical method. Therefore, it is important to know the best surgical method. Therefore, the purpose of this study is to introduce a case of recto-urethral fistula and a new surgical method in a 25-year-old man.
Case report: The patient was a 25-year-old man with complete urethra obstruction after PFUDD. The patient also mentioned the discharge of semen from the anus during sexual emission in sleep. The patient underwent flexible cystoscopy twice, which revealed no visible fistula. Then, the patient underwent posterior urethroplasty surgery, and during the release of the posterior canal, a 0.3 x 0.3 cm fistula was observed. The fistula was first completely freed from the surroundings. Then the freed bulbospongiosome muscle was brought longitudinally with the vascular base to the opening of the fistula as a covering tissue and finally quilted with vicryl.
Conclusion: The use of the posterior urethroplasty method and repair with the bulbospongiosome muscle flap provides acceptable treatment results for patients with RUF in the field of trauma. However, more research is needed regarding the evaluation of the patient’s sexual and urinary efficiency in order to obtain more accurate results.
Citation: Mirjalili A, Hosseini SM, Shojaeefar E, Abouei S. Posterior urethroplasty and recto-urethral fistula repair by bulbospongiosus muscle flap: A new surgical technique. J Clin Images Med Case Rep. 2023; 4(4): 2389.
Introduction
Recto Urethral Fistula (RUF) is a rare surgical condition requiring complicated and precise surgery. Culp and Calhoon classify recto urethral fistula into five etiological categories: A) congenital abnormality of the rectum and urinary tract, B) Iatrogenic after surgeries such as open prostatectomy, radiotherapy, Brachytherapy, urethral instruments, C) Trauma, D) Neoplasm, and E) Inflammatory. Of these, 60% of RUF are iatrogenic [2], and the majority of these are the cause of radical prostatectomy [3-5]. RUF has also been reported after prostate cryosurgery, radiotherapy, chemotherapy, high-intensity focused ultrasound, and transrectal hyperthermia [6-8]. Common symptoms of RUF are watery stools, fecaluria, and pneumaturia [9,10]. RUFs are diagnosed by symptoms such as fecaluria and pnematuria or leakage of urine from the rectum. Rectal digital examination, proctoscopy, and cystoscopy are some diagnostic methods [11,14]. Spontaneous closure of small RUFs following long-term urethral cauterization has been reported [15]. Currently, the accepted treatment protocol worldwide is surgical restoration [6,19], with more than 40 surgical techniques being described in the literature [17-19], including transperineal, transrectal, posterior pararectal, transabdominal and transvesticle, transsphincteric, or a combination of these [20]. However, to the best of our knowledge, no research has been conducted on the bulbspongenous muscle flap technique for the recto urethral fistula.
Case report
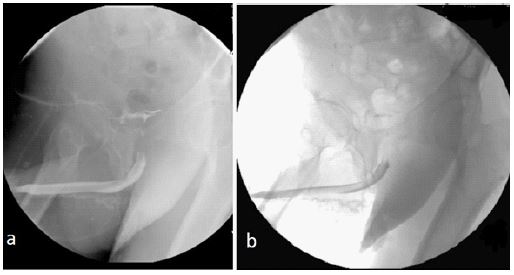
The patient was a 25-year-old man whose urethra was completely obstructed after PFUDD (pelvic fracture of urethral distraction disease) due to a car accident and trauma. The patient did not have any underlining disease and did not use any medication. After PFUDD, cystostomy was done. From the time of injury, the patient had erectile dysfunction and did not have a morning erection. Additionally, the patient reported semen fluid exiting from the anus during night orgasm. The patient underwent a flexible cystoscopy in the first attempt to correct this problem. The urethra was found to be one centimeter after Verumontanum, was completely obstructed, but no fistula was observed. The subsequent flexible cystoscopy also found no fistula and complete obstruction was seen (Figure 1).
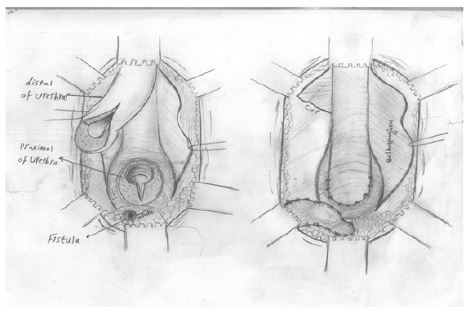
The patient underwent posterior urethroplasty surgery in which a perineal incision was made and the urethra was released and cut from the membranous obstruction site. While releasing the posterior urethra, a fistula opening measuring 0.3 x 0.3 cm was seen; a guide was passed from it entering the rectum to the distance of 3 cm from the posterior rectum sphincters. The fistula opening was released from the surrounding tissue and refreshed and repaired with vicryl thread 4-0. Following that, the hemi bulbospongiosus muscle was released and cut at the upper limit border, and a flap with a vascular base was quilted onto the fistula opening by vicryl 4-0. Finally, an end-to-end urethroplasty was done using 6 vicryl 3-0 sutures, and an urestomy was completed for the patient (Figure 2). In the follow-up (3-6 month), the patient had no recurrence of the fistula and no subsequent problems one month after discharge in his RUG (Figure 3). The patient was discharged from the hospital without any problems, although a more detailed examination of sexual problems and the functioning of the urinary system are required.

Discussion
RUF is a rare but devastating disease with many different etiologic origins, such as congenital, inflammatory, neoplastic, or traumatic [21]. Traumatic RUF is mainly seen in injuries sustained during war [22] and is accompanied by extensive damage to the urinary tract, which causes extensive constrictions. Traumatic RUF can cause challenging problems for surgical reconstruction. Because this condition is rare, no method has been proven more effective, becoming the accepted method of choice [22]. Closure of the RUF by itself or in a single-step technique is only possible in a few cases. In most cases, treatment is done in three steps, double diversion urinary and intestinal, closure technique, and undiversion. RUF repair includes many techniques, with the intersphincteric York-meson repair technique most commonly used [23]. Urologists tend to prefer the transperineal technique for RUF repair. This allows full exposure of the bladder neck and prostate and makes it possible for urethral repair after RUF repair. It also helps using different grafts. Interposition grafts are used as a second layer base after RUF closure to prevent relapse because of the closeness of the suture lines. Many types of interposition grafts are used in many different areas: gracilis muscle, dartus muscle, tunica vaginalis flap, penile skin, levator muscle, and bladder. The use of these tissue flaps is associated with complications such as hematoma formation, infections, and wound loss [24].
In this case study, we placed a bulbospongiosus flap on a patient with RUF, and the flap and fistula repair were successful. The advantages of using the bulbospongiosus muscle are A) it is well-vascularized, B) it is superficial and adjacent to the fistula and compared to other common flaps, its use is associated with a lower complication rate [25], and C) no functional impairment or cosmetic deformation at the repair site is seen. The bulbospongiosus muscle works as an erectile contraction muscle [26]. This function can be preserved post-operatively by the opposite bulbospongiosus and ischiocavernosus muscles. Using bulbospongiosus muscles, subcutaneous tissue, and skin is suggested [27]. However, this procedure may cause cosmetic deformation at the donor site. When the unilateral bulbospongiosus muscle flap is insufficient for the size of the fistula, a double-sided flap must be used. Since the width and length of the bulbospongiosus muscle are limited, if the fistula is huge in diameter or its position is too high, the use of the bulbospongiosus muscle flap (even bilaterally) may lead to tension in the sutures. In this situation, other flaps should be considered for repair [28,29].
Using the perineal approach of the penis to investigate possible fistulas, as previously stated in another study, can be useful [30]. Since it provides a complete examination of the urethra from the junction of the bulbomembrane to the glans, this approach makes it possible to accurately estimate the part of the urethra affected by the disease and facilitates proper removal of penile flap and grafting. Additionally, the allocation of flap and graft becomes technically easier. The second significant difference with previous studies is that the urethra was opened dorsally instead of ventrally after unilateral dissection. This approach has two important advantages. First, the vascular supply of the urethra and the bulbospongiosus muscle is preserved on one side, reducing the risk of ischemia and neurological dysfunction. Second, the ventral aspect of the corpus spongiosum is preserved. The corpus spongiosum is a vital blood supply source and supports the urinary tract. Lastly, after repairing the urethral fistula, the abdominal flap is covered with preserved corpus spongiosum, reducing the risk of diverticulum formation [30].
We acknowledge that our study presents a relatively short follow-up, which limits the number of complications that may occur after complex surgery, including fistula recurrence, diverticulum formation, or urinary dysfunction. Second, we also acknowledge that our study lacks information on sexual dysfunction before and after treatment. Indeed, erectile function scores and penile Doppler findings for our patients were not evaluated. Finally, we acknowledge that no conventional retrograde urethrogram was performed 12 months after surgery, as is now recommended by guidelines for complex cases [31]. In summary, our study joins previous publications on single-stage grafting with posterior ureteroplasty, expanding our knowledge of this challenging reconstructive surgery. Our approach proved that posterior uretroplasty with single-stage bulbospongiosus muscle grafting is an option for RUF fistula repair.
Conclusion
RUF fistula is a rare but devastating disease that poses a serious challenge to surgery, with no definitive surgical treatment method yet reported. This study found that the use of the posterior uretroplasty method and repair by bulbospongiosus muscle flap provided acceptable treatment results for patients with RUF due to trauma. However, more research is needed in fistula studies regarding the evaluation of the patient’s sexual and urinary efficiency in order to achieve more accurate results.
Declarations
Funding statement: Not funded.
Disclosure statement: All authors declare that there is “None”.
Data sharing statement: We confirm that all material methods and data are available.
Declaration of competing interest: The authors have no conflicts of interest.
Acknowledgments: We thank all those who participated in this study.
References
- Culp OS, Calhoon HW. A variety of recto urethral fistulas: Experiences with 20 cases. J Urol. 1964; 91: 560–571.
- Crippa A, Dall’Oglio MF, Nesrallah LJ, Hasegawa E, Antunes AA, Srougi M, et al. The York-Mason technique for recto-urethral fistulas. Clinics. 2007; 62: 699–704.
- Tiptaft RC, Motson RW, Costello AJ, Paris AME, Blandy JP, et al. Fistulae involving rectum and urethra: the place of Parks operations. Br J Urol. 1983; 55: 711–715.
- Noldus J, Graefen M, Huland H. An ‘old technique’ for a new approach for repair of rectourinary fistulas. J Urol. 1997; 157: 1547.
- Eastham JA, Scardino PT. Radical Prostatectomy. In: Walsh PC, Retik AB, Vaughan ED, Wein AJ, editors. Campbell’s Urology. 7th ed. Philadelphia: WB Saunders Co.; 1997; 2554.
- Zippe CD. Cryosurgery of the prostate: technique and pitfalls. UrolClin North Am. 1996; 23: 147–163.
- Andrews EJ, Royce P, Farmer KC. Transanal endoscopic microsurgery repair of rectourethral fistula after high-intensity focused ultrasound ablation of prostate cancer. Colorectal Dis. 2011; 13: 342–343.
- Montorsi F, Guazzoni G, Bergamaschi F, et al. Transrectal prostatic hyperthermia and advanced prostatic cancer. Clinical results of one year follow up. ActaUrol Ital. 1992; 6: 471–474.
- Nyam DC, Pemberton JH. Management of iatrogenic rectourethral fistula. Dis Colon Rectum. 1999; 42: 994–997.
- Kitamura H, Tsukamoto T. Rectourinary fistula after radical prostatectomy: review of the literature for incidence, etiology, and management. Prostate Cancer. 2011: 629105.
- Blandy JP, Singh M. Fistulae involving the adult male urethra. Br J Urol. 1972; 44: 632–643.
- Chiou RK, Anderson JC, Tran R, et al. Evaluation of urethral strictures and associated abnormalities using resolution and color Doppler ultrasound. Urology. 1996; 47: 102–107.
- Al-Ali M, Kashmoula D, Saoud IJ. Experience with 30 posttraumatic rectourethral fistulas: presentation of posterior transsphincteric anterior rectal wall advancement. J Urol. 1997; 158: 421–424.
- Noldus J, Graefen M, Huland H. An ‘old technique’ for a new approach for repair of recto urinary fistulas. J Urol. 1997; 157: 1547.
- Chun L, Abbas MA. Rectourethral fistula following laparoscopic radical prostatectomy. Tech Coloproctol. 2011; 15: 297–300.
- Hanus T. Rectourethral fistulas. Int Braz J Urol. 2002; 28: 338–345.
- Thomas C, Jones J, Jäger W, Hampel C, Thüroff JW, Gillitzer R, et al. Incidence, clinical symptoms and management of rectourethral fistulas after radical prostatectomy. J Urol. 2010; 183: 608–612.
- Hanna JM, Turley R, Castleberry A, et al. Surgical management of complex rectourethral fistulas in irradiated and nonirradiated patients. Dis Colon Rectum. 2014; 57: 1105–1112.
- Rouanne M, Vaessen C, Bitker MO, Chartier-Kastler E, Rouprêt M, et al. Outcome of a modified York Mason technique in men with iatrogenic urethrorectal fistula after radical prostatectomy. Dis Colon Rectum. 2011; 54: 1008–1013.
- Dal Moro F, Mancini M, Pinto F, Zanovello N, Bassi PF, Pagano F, et al. Successful repair of iatrogenic rectourinary fistulas using the posterior sagittal transrectal approach (York-Mason): 15-year experience. World J Surg. 2006; 30: 107–113.
- Culp OS, Calhoon HW. A variety of rectourethral fistulas: Experiences with 20 cases. J Urol. 1964; 91: 560–571.
- Al-Ali M, Kashmoula D, Saoud IJ. Experience with 30 posttraumatic rectourethral fistulas: Presentation of posterior transsphincteric anterior rectal wall advancement. J Urol. 1997; 158: 421–424.
- Fengler SA, Abcarian H. The York Mason approach to repair of iatrogenic rectourinary fistulae. Am J Surg. 1997; 173: 213–217.
- Rajaian S, Rajadoss MP, Nayak S, Kekre NS. Traumatic rectourethral fistula repair: A potential application of porcine small intestinal submucosa. Indian J Urol. 2013; 29: 148-150.
- Rangnekar NP, Imdad Ali N, Kaul SA, Pathak HR. Roleof the Martius procedure in the management of urinary-vaginal fistulas. J. Am. Coll. Surg. 2000; 191: 259–63
- Langman J, Woerdeman MW. Atlas of Medical Anatomy. W.B. Saunders Company, Philadephia, 1978; Pelvis-P39
- Angioli R, Penalver M, Muzii L et al. Guidelines of how to manage vesicovaginal fistula. Crit. Rev. Oncol. Hematol. 2003; 48: 295–304.
- Dmochowski R. Surgery for vesicovaginal fistula, urethrovaginal fistula, and urethral diverticulum. In: Walsh PC, Retic AB, Vaughan ED, Wein AJ (eds). Campbell’s Urology, 8th edn. Elsevier Science, Philadelphia, 2002; 1195– 203.
- Smith GL, Williams G. Vesicovaginal fistula. BJU Int. 1999; 83: 564–570.
- S Kulkarni, G Barbagli, D Kirpekar, F Mirri, M Lazzeri.Lichen sclerosus of the male genitalia and urethra: Surgical options and results in a multicenter international experience with 215 patients. Eur Urol. 2009; 55: 945-954.
- F Campos-Juanatey, NIOsman, T Greenwell, et al. European Association of Urology guidelines on urethral stricture disease (part 2): Diagnosis, perioperative management, and follow-up in males Eur Urol. 2021; 80: 201-212.