
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 4
A therapeutic challenge in an elderly woman and spectacular
clinical response to an unusual left supra-clavicular metastasis
of ovarian adenocarcinoma
Mohammed El Fadli1; Ganiou Adjadé1*; Kelly Haag1; Ismail Essadi2; Rhizlane Belbaraka1
1Department of Medical Oncology, Mohammed VI university hospital, University of Cady Ayyad, Marrakech, Morocco.
2Department of Medical Oncology, Avicenna Military Hospital, University of Cady Ayyad, Marrakech, Morocco.
*Corresponding Author : Ganiou adjade
Department of Medical Oncology, Mohammed VI university hospital, University of Cady Ayyad,
Marrakech, Morocco.
Tel: +212600592141;
Email: Ganiou.adjade@gmail.com
Received : May 02, 2023
Accepted : May 26, 2023
Published : Jun 02, 2023
Archived : www.jcimcr.org
Copyright : © Adjade G (2023).
Abstract
Ovarian carcinomas with a single left supraclavicular metastasis in the node of Virchow are rare. We report a case of an 80-year-old woman with a large painful left supraclavicular adenopathy. Immunohistochemical study of the lymph node biopsy and pelvic magnetic resonance imaging revealed adenocarcinoma of ovarian origin. After three courses of full-dose carboplatin-based chemotherapy, we observed the disappearance of the left supraclavicular mass, normalization of the CA 125 marker, and a clear decrease in the size of the right adnexal mass. This case informs us about exceptional locations of ovarian carcinomas, the good tolerance of elderly subjects to therapeutic standards in terms of chemotherapy, and the possibility of making certain metastatic tumors curable.
Keywords: Virchow’s node; Ovarian adenocarcinoma; Metastasis; elderly; Morocco.
Citation: Fadli ME, Adjadé G, Haag K, Essadi I, Belbaraka R. A Therapeutic challenge in an elderly woman and spectacular clinical response to an unusual left supra-clavicular Metastasis of ovarian adenocarcinoma. J Clin Images Med Case Rep. 2023; 4(6): 2439.
Clinical image description
Our patient is 80 years old and under treatment for hypertension and cardiac arrhythmia due to atrial fibrillation. She presented with a painful left cervical adenopathy that gradually increased in size over 12 months. Clinical examination revealed a patient in good general condition with an erythematous poly-lobed mass, tender to palpation, occupying the left supraclavicular region (Figure 1A). Cervicothoracic Computed Tomography (CT) described a left supraclavicular mass measuring 8.8 x 9.3 cm and compressing the jugulocarotid axis (Figure 2A). On pathological examination, it was a poorly differentiated adenocarcinoma with immunohistochemical expression of anti-CK7, anti-CK19, anti-WT1, anti-PAX8 antibodies and an absence of expression of anti-CK20, anti-CDX2, anti-GATA3, anti-P40 antibodies, pointing to a gynecological origin (Figure 1B). An abdominal-pelvic CT scan and pelvic Magnetic Resonance Imaging (MRI) revealed a 3.9 x 4 cm heterogeneous right lateral uterine mass (Figure 3A). Associated lateropelvicadenopathies were measuring 20 x 27 mm on the right and 12 x 14 mm on the left. The CA125 marker was elevated to 944 U/ml. She received three courses of chemotherapy every three weeks combining Carboplatin AUC5 at Day 1 (D1) with weekly Paclitaxel 80 mg/m² at D1, D8, and D15 with very good tolerance. No dose reduction was required due to his age and cardiac history. A post-chemotherapy evaluation revealed a spectacular clinical response with the disappearance of the supra-clavicular adenopathy (Figure 1C) and normalization of CA125 (12.93 IU/mL). On the follow-up CT scan, there was complete regression of the left supraclavicular mass (Figure 2B) and a decrease in the right adnexal mass size, 2.3 x 2.9 cm vs 3.9 x 40 cm (Figure 3B). She subsequently underwent a hysterectomy with bilateral adnexectomy.
This case informs us about exceptional locations of ovarian carcinomas, the good tolerance of elderly subjects to therapeutic standards in terms of chemotherapy, and the possibility of making certain metastatic tumors curable.
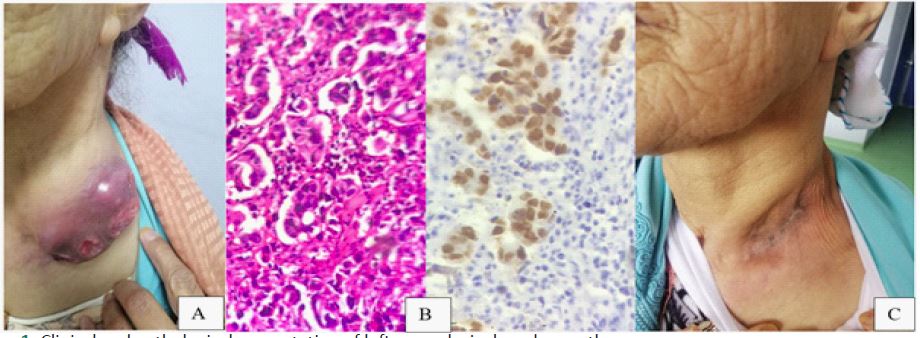
(A) Appearance of the initial large left supra-clavicular adenopathy.
(B) Pathological and Immunohistochemical aspect with antiPAX 8 antibodies positive appearance (HEx10).
(C) Clinical Disappearance of adenopathy after chemotherapy.
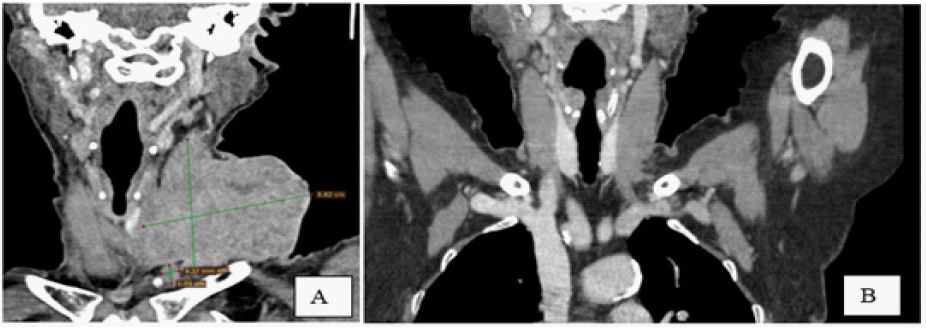
(A): Large initial supraclavicular mass.
(B): Disappearance of adenopathy after chemotherapy.
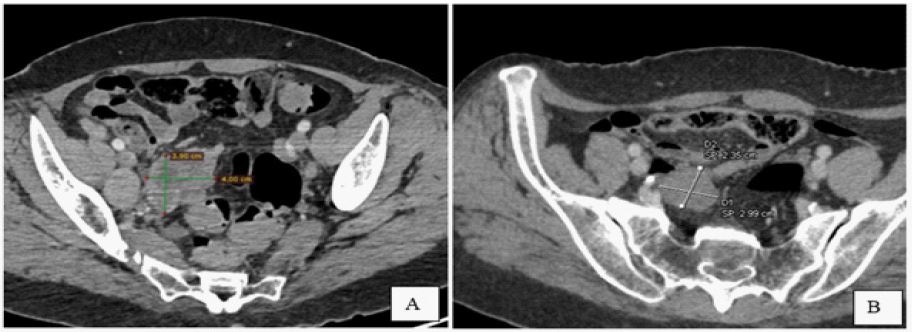
(A) Initial appearance of the left ovarian mass.
(B) Reduction in size of the mass after chemotherapy.