
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 4
Human umbilical cord blood-derived mesenchymal stem cells therapy for cerebral infarction in animal model: A meta-analysis
Mijuan Zhang1*; Zhanning Qi1; Tao Wang2; Wenjin Yu1; Jing Zhang1
1Department of Neurology, Xianyang Hospital of Yan’an University, Xianyang City, Shaanxi Province, China.
2Department of Neurology, Shaanxi Province People′s Hospital, Xi’an City, Shaanxi Province, China.
*Corresponding Author : Mijuan Zhang
Xianyang Hospital of Yan’an University, Xianyang City, Shaanxi Province, China.
Email: 1359801925@qq.com
Received : Sep 08, 2023
Accepted : Sep 26, 2023
Published : Oct 03, 2023
Archived : www.jcimcr.org
Copyright : © Zhang M (2023).
Abstract
Aim: Cerebral infarction (CI) is a serious cerebrovascular infarction disease. In recent years, the use of human umbilical cord blood-derived mesenchymal stem cells (hUCB-MSCs) has received attention as a new alternative for treating CI in animal model. This systematic review evaluated the efficacy and safety of hUCB-MSCs, using as a treatment in improving functional recovery of CI in animal model.
Methods: Electronic databases through July 5, 2023 were searched to identify relevant studies that controlled hUCB-MSCs treatment studies focusing on CI in animal model. We independently selected and assessed the relevant studies.
Results: 27 studies that fulfilled the inclusion criteria were included. Compared with control group, significant beneficial effects were observed in hUCB-MSCs group regarding the neurological deficit scores (mean difference [MD]: −1.57, 95% confidential interval [CI]: −2.06, −1.08, P<0.00001), infarct size (MD: −2.82, 95% CI: −4.14, −1.49, P<0.0001).
Conclusions: The results indicated that hUCB-MSCs treatment can promote functional recovery and reduce infarction for CI in animal model.
Keywords: Cerebral infarction; Human umbilical cord blood-derived mesenchymal stem cells; Effectiveness; Meta-analysis.
Citation: Zhang M, Qi Z, Wang T, Wenjin Yu W, Zhang J. Human umbilical cord blood-derived mesenchymal stem cells therapy for cerebral infarction in animal model: A Meta-Analysis. J Clin Images Med Case Rep. 2023; 4(10): 2625.
Introduction
Cerebral infarction (CI) is a serious cerebrovascular infarction disease, which refers to a clinical event in which circulatory disturbances in the cerebral arteries lead to tissue ischemia and hypoxia and cause cerebral dysfunction rapidly [1]. CI has a high incidence, mortality and disability rate, and it has become a common disease that threatens human health and life expectancy [2,3]. The American Heart Association estimates that by the year 2030 there will be an increase adults developing stroke in the United States, a projected increment of 20.5% from 2012 [4]. Despite vigorous studies published during the last decades, treatment opportunities are still limited. At present, there are many therapeutic methods for CI, including antiplatelet therapy, anticoagulant therapy, brain protective agents, intravenous thrombolysis, intravascular thrombolysis and so on [5]. Among them, intravenous thrombolysis and intravascular thrombolysis are the most effective methods to treat patients with CI [6,7], but they are limited by a narrow time window. Within this time window, therapeutic efficacy is reduced continuously, accompa nied by an increasing probability of serious complications such as hemorrhages [8]. Once brain cells die, the damage to the central nervous system is permanent. Therefore, these methods are suboptimal for functional recovery after injury.
Mesenchymal stem cells (MSCs) exist in almost all tissues, including spleen, muscle, bone marrow, placenta, dermis, umbilical cord, and so on [9]. Placenta and umbilical cord are known as the abundant sources of MSCs [10]. When a population called the umbilical cord matrix MSCs is isolated for the first time, it is demonstrated that these cells have the ability of self-renewal and high proliferation [11]. Moreover, in vitro, MSCs do not induce proliferative response of allogeneic lymphocytes, because they are not immunogenic. According to the available evidence, human umbilical cord blood-derived mesenchymal stem cells (hUCB-MSCs) have remarkable characteristics including availability, being immunosuppressive, differentiation to other cell lines, being easy to isolate and expand, being safe from malignant formation, and the possibility of auto-graft and allograft which make them a better candidate for clinical applications of stem cell-based therapies [13]. In recent years, the use of hUCB-MSCs has received attention as a new alternative for treating CI in animal model. Many animal studies have shown that MSCs have great potential to serve as therapeutic agents for stroke treatment. MSCs in an ischemic area of the rat brain can differentiate into nerve cells and improve the recovery of nerve function [14,15] and it can improve neurological deficits in stroke [16]. A study [17] also proved that the transplanted umbilical cord stem cells in an animal model of stroke improved the neurological deficits through the secretion of neurotrophic growth factors. Another study [18] demonstrated that intravenous administration of hUCB-MSCs after stroke can reduce infarction. However, the design projects, including hUCB-MSCs type, dose, number, route, and time interval, in each research are so different that the final therapeutic effect is difficult to evaluate. As a result, the best way of hUCB-MSCs therapy remains unclear.
Therefore, we performed this meta-analysis to evaluate the efficacy and safety of hUCB-MSCs as a treatment in improving functional recovery of CI in animal model, to determine if the evidence from the animal studies of hUCB-MSCs supports its use in clinical practice.
Materials and methods
Literature search and inclusion criteria
Two researchers independently and systematically searched numerous electronic bibliographic databases, including PubMed, Embase, and Wanfang, and China National Knowledge Infrastructure by the end of July 5, 2023. There were no restrictions on the language of publication in this search. This article was performed through using relevant guidelines [19] to select relevant studies between hUCB-MSCs and cerebral infarction. The following searching strategy was used: (“cerebral ischemia” OR “cerebral infarctions” OR “ischemic stroke” OR “ischemic cerebrovascular disease”) AND (“human umbilical cord blood-derived mesenchymal stem cells” OR “umbilical cord blood mesenchymal cells” OR “hUCB-MSCs”). During the retrieval process, the two researchers independently searched and cross-checked the result, and discussed in disagreements, and the third researcher consulted if necessary.
Inclusion criteria: (1) Studies on animal model without restriction of species, sex, and modeling methods; (2) The treatment group received monotherapy with hUCB-MSCs, and the control group received the same amount of nonfunctional substances or no treatment; and (3) Studies evaluating the effect of hUCB-MSCs therapy CI in animal model, such as the neurological deficit scores and infarct size.
Exclusion criteria: (1) Studies in vitro studies and human subjects; (2) Studies combined with other therapies; (3) Studies lacked relevant data; (4) Studies without a separate control group; and (5) Case reports, reviews, and duplicate publications.
Data extraction and methodological quality appraisal
To determine if a study should be included, two researchers independently searched the retrieved studies. We extracted the relative data using the pre-designed table and cross-checked the results. When faced with conflicts, we together discussed, and the third researcher negotiated if necessary. For each study, the following data were extracted: first author, year of publication, animal characteristics (species, sex, age), intervention details (dose, number, timing and route of hUCB-MSCs transplantation), follow-up visit (observation time of outcomes after hUCB-MSCs therapy), measured the correlation with our primary outcomes, and research type. If only figures were presented in some studies, GetData Graph Digitizer software version 2.22 was used to extract the data. According to the Cochrane Hand-book for Systematic Reviews of Interventions (CHSRI) [20], we chose to combine the results of different subgroups into one treatment group for analysis to address the issue of the classification of the therapeutic drugs into subgroups in the original study.
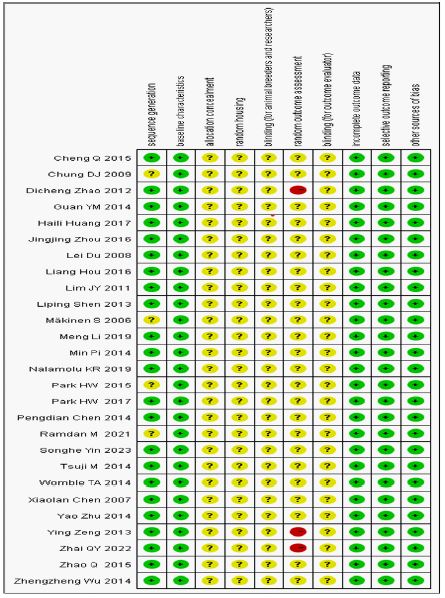
We assessed the quality of the animal studies using the SYstematic Review Center for Laboratory animal Experimentation (SYRCLE) risk-of-bias tool [21]. The assessment content covered deviations in ten areas, and each item was scored as one point. Each item was as follows: (a) sequence generation, (b) baseline characteristics, (c) allocation concealment, (d) random housing, (e) blinding (for animal breeders and researchers), (f) random outcome assessment, (g) blinding (for outcome evaluator), (h) incomplete outcome data, (i) selective outcome reporting, and (j) other sources of bias. Disagreements between the researchers were discussed and resolved through a discussion with the third researcher (Tao Wang).
Data analysis
All data were meta-analyzed using RevMan 5.4 provided by Cochrane collaboration. All variables were continuous data, and a standard deviation (SD) and 95% confidence interval (CI) were used to indicate the effect size. Statistical heterogeneity was expressed by I2 statistics. When I2 statistics was less than 50%, heterogeneity was small and acceptable, and we used the fixed effect model for meta-analysis. When I2 statistics was more than 50%, heterogeneity was relatively large, and then the reason for high heterogeneity can be speculated by sensitivity analysis or subgroup analysis. Meanwhile, the random effect model can be used for meta-analysis. Funnel plots were used to examine for any potential publication bias in the studies.
Results
Description of studies
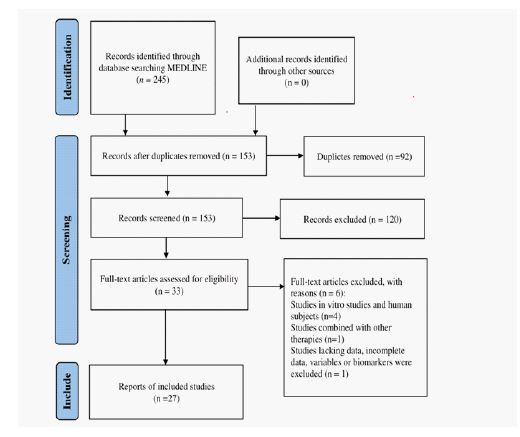
The detailed selection process was illustrated in Figure 1. We initially searched 245 literatures during the searching of electronic database. Among them, 218 literatures were excluded after an intensive screening of the titles, abstracts, and the full text of relevant studies and so on. Finally, 27 articles [22-48] were included, including 14 Chinese [22-35] and 13 English articles [36-48].
All animal models included in the studies were rats, mice, rabbits or beagles, including non-rodents (rabbits and beagles) used in 3 studies [28,37,39] and rodents (rats and mice) used in 24 studies. In terms of gender, 1 study [37] was not mentioned, one study [40] was male and female animal model, and the rest were male animal model. 4 studies [22,36,40,43] mentioned the age of the experimental animals, ranging from postnatal day 12 to 3-4 months, and 12 [25,29-31,37,38,41,42,44-46,48] studies mentioned the animals as adult. In addition, the data representing the dose, transplantation number and transplantation time of hUCB-MSCs were different among studies. In terms of transplantation route, there are tail vein, femoral vein, intranasal, intracerebral, basilar artery, intrathecal, penile vein, and intracarotid artery. Except for 2 studies [36,41] that didn’t mention it, the time of the last outcomes ranged from 24 hours to 6-7 weeks. Regarding primary outcomes, 15 studies reported infarct size, 24 reported he neurological deficit scores, including NSS, Purdy, mNSS, Zea-Longa and Rotrarod test. Detailed characteristics of the included studies were listed in Table 1.
Methodological quality of included studies
Each risk of bias item of all articles was shown in Figure 2. None of the studies fulfilled all ten criteria for low risk of bias. Of the 27 included studies, 23 studies described the methods used to generate the allocation sequence, while 4 studies [36,37,44, 47] lacked information about this process, and the risk of bias was judged to be “unclear risk” (a). Studies demonstrated similar baseline characteristics between the hUCB-MSCs group and control group (b). Because of the special properties of hUCB-MSCs administration, it was difficult for researchers to achieve a blinding procedure when acquiring hUCB-MSCs, although this wasn’t influence the experimental results. The risk of bias was unclear for all articles across the domains of allocation concealment, random animal housing, and random outcome (c,d,e,g). In terms of randomization and blinding of outcome evaluation, 4 studies [24,25,48] described that animals were not randomly selected to assess outcomes, defined as “high risk”. And the remaining studies were defined as “unclear risk” (f). Incomplete results data were adequately treated in almost all studies (h). Regarding the reporting of biases, no risk was identified in the selected studies (i). Other potential sources of bias weren’t identified in any of the articles (j).
Data analysis
Effects on the neurological deficit scores
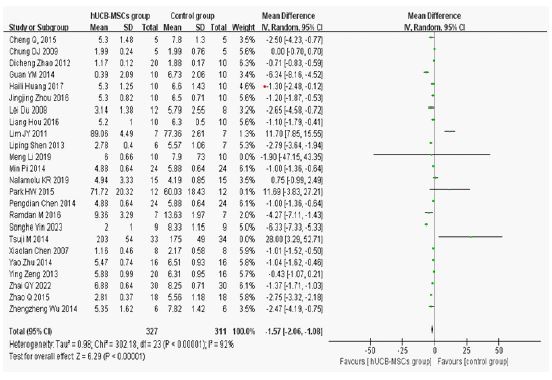
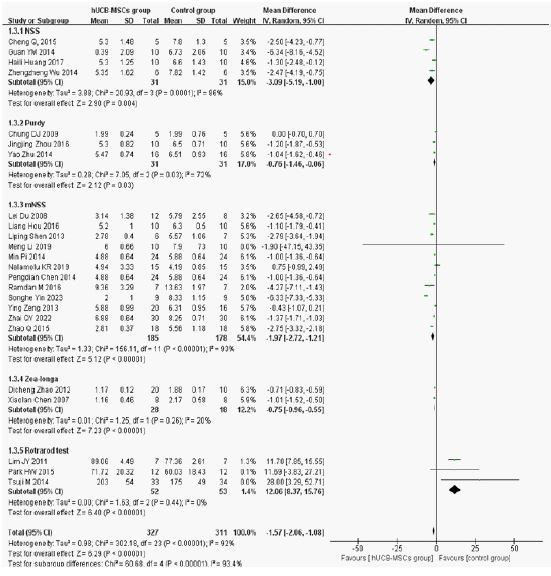
The neurological deficit scores were measured in most studies included in our review. As shown in Figure 3, the MD was −1.57 (95% CI: −2.06, −1.08, P< 0.00001), suggesting significant lower the neurological deficit scores in the hUCB-MSCs group compared to the control group. Because of the high heterogeneity (I2=92%, P< 0.00001), we used the sensitivity analysis, and we did not find a reason for the high heterogeneity. AccordAccording to the different of the neurological deficit scores items, the objects of study were classified into NSS (MD: −3.09, 95% CI: −5.19, −1.00, P=0.004), Purdy (MD: −0.76, 95% CI: −1.46, −0.06, P=0.03), mNSS (MD: −1.97, 95% CI:−2.72, −1.21, P< 0.00001), Zea-longa (MD: −0.75, 95% CI: −0.96, −0.55, P< 0.00001), and Rotrarod test (MD: 12.06, 95% CI: 8.37, 15.76, P< 0.00001) (Figure 4).
Effects on infarct size
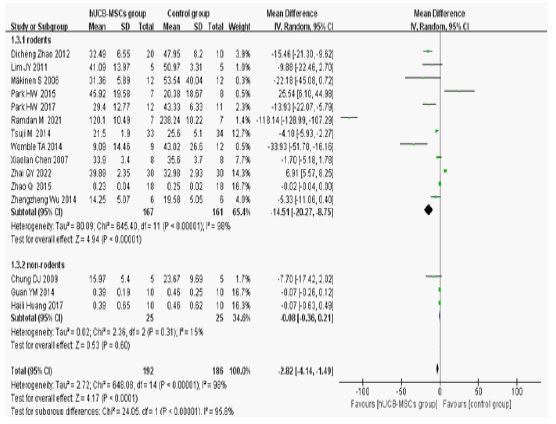
Compared to the control group, the infarct size was significantly decreased in the hUCB-MSCs group as shown in Figure 5 (MD: −2.82, 95% CI: −4.14, −1.49, P< 0.0001).
Because of the high heterogeneity (I2 =98%, P< 0.00001), we used the sensitivity analysis, and we didn’t find a reason for the high heterogeneity. According to the different animal species, the objects of study was classified into rodents (MD: −14.51, 95% CI: −20.27, −8.75, P< 0.00001), and non-rodents (MD: −0.08, 95% CI: −0.36, −0.21, P=0.60) (Figure 6).
Publication bias
In terms of the neurological deficit scores, we found no publication bias in the meta-analysis (Figure 7). In terms of infarct size, it likely affected by publication bias (Figure 8). One included studies [48] mainly causes publication bias. We searched all published articles as thoroughly as possible, but publication bias was still unavoidable. After analysis, we found that the objects of this study were rodents, and subgroup analyses suggested that animal species may be the source of heterogeneity. There was no special effect on infarct size for CI in animal model whether it was rodents or not, so it has no major impact on the research results of this article.
Table 1: Characteristics of included studies.
| StudyID | Animalmodel | dose,number; timing of transplantation | Transplantationroute | Observationtime of outcomes | Primaryoutcomes | Researchtype |
|---|---|---|---|---|---|---|
| XiaolanChen [22] 2007 | 3month old male SD rats | 3×106/ml; single injection; 30minutes after moding | Tail vein | 28days | Zea-longa; infarct size | RCT |
| LeiDu [23] 2008 | HealthymaleSD rats | 3×106/ml; single injection; 24 hours after MCAO | Intracerebral | 28days | mNSS | RCT |
| DichengZhao [24] 2012 | Male SD rats | 5×106/cells; single injection; 30minutes after moding | Tail vein | 28 days | Zea-longa;infarct size | RCT |
| YingZeng [25] 2013 | Healthyadult male rats | 3×106/ml; single injection;24 hours after molding | Tail vein | 28days | mNSS | RCT |
| LipingShen [26] 2013 | MaleSD rats | NR; multipleinjection;24hours after molding | Intranasal | 14 days | mNSS | RCT |
| ZhengzhengWu [27] 2014 | Malemouse | 4×106/ml;single injection; 30minutes after moding | Tailvein | 7days | NSS;infarct size | RCT |
| YaoZhu [28] <2014 | Healthy male rabbits | 5×106/cells; single injection; immediatelyafter moding | Femoralvein | 14days | Purdy | RCT |
| PengdianChen [29] 2014 | Healthyadult male SD rats | 1×106/μl; single injection;24hours after molding | Intracerebral | 28days | mNSS | RCT |
| MinPi [30]2014 | Adultmale SD rats | 1×105/μl; single injection; 2 days after molding | Intracerebral | 28days | mNSS | RCT |
| LiangHou [31] 2016 | Adultmale SD rats | 1×106/cells;single injection; 10minutes after molding | Tailvein | 28days | mNSS | RCT |
| JingjingZhou [32] 2016 | HealthymaleSD rats | 1×106/cells; single injection;10minutes after molding | Tail vein | <14days | | RCT |
|
| HailiHuang [33] 2017 | Healthymale rabbits | 1×109 /m; single injection; 24hours after molding | Femoral vein | 14days | NSS; infarct size | RCT |
| MengLi [34] 2019 | MaleSD rats | 1×106 /cells; single injection; 2 days after molding | Tailvein | 14days | mNSS; | RCT |
| SongheYin [35]2023 | MaleSD rats | 1×106 /cells; single injection; 24 hours after molding | Tailvein | 7days | mNSS | RCT |
| Mäkinen S [36] 2006 | MaleWistar rats (3–4 months) | 1-5×107 cells;single injection; 24 hours after MCAO | Intravenous | NR | Infarctsize | NR |
| Chung DJ [37] 2009 | Tenadult beagles | 1×106/ml;single injection; 1 day after moding | Basilarartery | 14and 28 days | Purdy;infarct size | NR |
| Lim JY [38] 2011 | Seventy-fouradult male rats | 1×106, 5× 105, 1× 105cells; single injection;NR | Tailvein and intrathecal | 28days, | Rotarodtest; infarct size | RCT |
| Guan YM [39] 2014 | Malerabbits | 1×106/ml;single injection; several minutes after MCAO | Femoralvein | 14days | NSS;infarct size | RCT |
| Tsuji M [40] 2014 | postnatalday 12 male and female mousepups |
1×105 cell; single injection; 48 hours after stroke | Femoralvein | 6and7weeks | Rotarodtest, infarct size | RCT |
| Womble TA [41] 2014 | Adultmale SD rats | 1 ×10 6cells;singleinjection; 48 hours post-MCAO | Penilevein | NR | Infarctsize | RCT |
| Zhao Q [42] 2015 | Adultmale rats | 1×104cells/cm2;multiple injection; 24 hours after MCAO | Intranasal | 14days | mNSS;infarct size | RCT |
| Cheng Q [43] 2015 | 6–7-week-oldmale mice | 4×106/ml;single injection; 30 minutes after moding | Tailvein | 7days | NSS | NR |
| Park HW [44] 2015 | Adultmale SD rats | 5×105cells;singleinjection;48 hours after MCAO | Intracerebral | 28and30days | Rotarodtest; infarct size | NR |
| Park HW [45] 2017 | Adultmale SD rats | 5×105 cells; single and double;2 and 9 days after MCAO | Intracranial | 28days | Infarctsize | RCT |
| >Nalamolu KR [46] 2019 | Healthyadult male SD rats | NR | Tailvein | 7 days | mNSS | RCT |
| RamdanM [47] 2021 | Wistarmale rats | NR;24 h after the MCAO | Intracranial | 24hours | mNSS; infarct size | NR |
| Zhai QY [48] 2022 | Adultmale SD rats | 1×106/ml;single injection; immediately after reperfusion | Intra-arterial | 7days | mNSS;infarct size | RCT |
NSS: Neurological severity scores; RCT: Randomized controlled trial; mNSS: Modified neurological severity scores; SD: Sprague–Dawley;
MCAO: Middle cerebral artery occlusion; NR: Not reported;
Follow-up (days) suggests the observation time of outcomes after mesenchymal stem cell administration
 :low risk;
:low risk;  : unclear risk;
: unclear risk;  : high risk
: high risk



Discussion
Over the years, many epidemiological studies have been published on hUCB-MSCs therapy for CI in animal model. Laboratory animals are widely used to evaluate the medication’s efficacy. The biological similarity to humans is one of the most important characteristics of laboratory animals such as mice and rats [49]. Thus, in most experimental CI studies, these animals are preferred. Our meta-analysis evaluated the efficacy and safety of hUCB-MSCs therapy for CI in animal model. The results indicated that hUC-MSCs treatment can promote functional recovery and reduce infarction in animal model of CI. This will provide more possibilities for hUCB-MSCs therapy in preclinical studies of CI.
At present, the exact mechanism of hUCB-MSCs therapy for CI in animal model remains unclear. It may be in the following ways: (1) Angiogenesis and vascular stabilization [17]: Treatment of CI in animals model with hUCB-MSCs increase the expression of endogenous angiogenic factors, enhance the proliferation of vascular endothelial cells, and promote the regeneration of blood vessels in ischemic brain tissue [50]. Studies have found that hUCB-MSCs treatment increased expression of Angiopoietin-1, contribute to vascular remodeling in the ischemic brain which plays an important role in functional outcome after CI [39,51]. (2) Peripheral immune inflammatory response [40]: During cerebral ischemia, damaged cells and extracellular peroxiredoxin activate infiltrate macrophages, leading to the release of inflammatory cytokines such as interleukin (IL)-1. Therefore, injured brain cells and impregnated leukocytes produce various inflammatory cytokines and mediators that aggravated post-ischemic inflammation and injury [52]. HUCB-MSCs treatment can significantly reduce the increase of serum IL-1β, and IL-6 caused by cerebral ischemia, increase the content of anti-inflammatory cytokine in serum and focal ischemic brain tissue, and alleviate local immune inflammatory response [53, 54]. (3) Inhibit apoptosis: When brain tissue is damaged, excitatory amino acids are secreted into extracellular fluid in large quantities, and free radical damage caused by oxidative stress persists. Animal studies [55] have confirmed that hUCB-MSCs transplanted into cerebral ischemia-reperfusion rabbits can significantly reduce nerve cell death and significantly restore nerve function in cerebral tissue in focal ischemic area (4). Nutritional support mechanism: hUCB-MSCs release neurotrophic factors to support the survival of surviving cells in the ischemic penumbra, repair synaptic function and promote angiogenesis [56].
Usually, animal studies are relevant to clinical application and used to evaluate the efficacy and safety of hUC-MSCs therapy. In Guan YM [41] study, no influence was found on complete blood counts, serum glucose, liver function or renal function in middle cerebral artery occlusion (MCAO) rabbits at 24 h and 2 weeks after transplantation, suggesting that intravenous infusion of hUCB-MSCs was safe for rabbits in the short-term. As far as we know, several clinical trials have been conducted to explore the potential benefits of hUCB-MSCs transplantation for CI patients [57,58]. A phase clinical trial [57] reported that an adult patient with hemiplegia due to ischemic stroke significantly improved within 12 months after receiving allogeneic hUCB-MSCs therapy. Except for 1 case of hypothermia in treatment group, the transplanted route of up to 3×107 cells MSCs was safe in 100 patients with CI. In the patient with a fever, the symptoms were quickly relieved after symptomatic treatment. Another clinical trial [58] indicated that 30 ml of hUCB-MSCs is injected once every 5 days for a total of six times, which improved the symptoms of CI patients after 1 month. Even though in these clinical trials, hUCB-MSCs therapy is a generally safe and promising candidate to slow the disease progression. The success of hUC-MSCs therapy is partly reliant on the appropriate method and timing of hUCB-MSCs injection. Study [44] indicated that hUCB-MSCs by lumbar puncture intrathecal injection was an attractive and potentially successful method and may be a clinically feasible means of providing less invasive and repeatable transplantation therapy, but this method of injection was known to be more invasive than intra-arterial or intravenous methods, and therefore, clinical application seems to be implausible at this point. Intravenous infusion of cells is comparatively the least invasive approach [59]. Furthermore, beneficial effects of hUC-MSCs administered within 72 hours after MCAO are clearly shown. The failure to induce sustained functional recovery, lesion size reduction, and limitation of glial scaring in animals treated 120 h following MCAO and thereafter indicates a time window of at least 72 h for efficient cell application [60]. Regardless of the type of donor, intra-parenchymal administration of hUCB-MSCs results in significant therapeutic effects in the ischemic brain [42]. However, the sample size of this subgroup analysis is small, and there may be false-positive or false-negative conclusions.
We attempted to explore the heterogeneity from animal species, intervention details, follow-up visit, measured the correlation with our primary outcomes, and so on. According to subgroup analysis, we found that the possible contributor of heterogeneity was the animal species and different scales of nerve deficit score. We haven’t found that the likely contributors to heterogeneity were the animal model, hUCB-MSCs type, hUCB-MSCs dose, and so on. Our study also had some advantages. First, the inherent advantages of meta-analysis were seen. It overcame selective and potentially biased inclusion studies and weighing of studies results when explaining the evidence. This made the combined results even more reliable and convincing. Secondly, we performed a systematic literature search, comprehensive data collection, which can improve the accuracy of our findings. Finally, the main results about neurological deficit scores and infarct size could provide vital insight into the future study. It was of great significance for finding a new way to treat CI. However, the limitations of our study should be admitted. Firstly, due to the differences in the design, the results of the combined analysis may not be rigorous. Secondly, the included studies were limited to those that had been published. The outcomes will be altered when undocumented data are published. As expected, studies reporting positive results were easier to publish, especially in animal studies. Finally, considerable heterogeneity remained in the studies evaluated in the subgroup analysis, because it is usually difficult to avoid heterogeneity. In addition, despite our efforts to avoid publication bias publication bias occurred, which needed to be considered when interpreting the study outcomes.
Conclusion
In conclusion, this meta-analysis evaluates the efficacy and safety of hUCB-MSCs therapy on the neurological deficit scores and infarct size in animal model, which provides an important basis for future translational clinical studies. However, considering the limited application of animal studies to humans, the heterogeneity existing between studies, the results should be extrapolated to the clinical setting with great caution. The long-term efficacy and safety of hUCB-MSCs in CI patients still require additional substantiation. In the future, large sample, andomized controlled trials are required to prove the efficacy and safety of hUCB-MSCs therapy for CI.
Declarations
Ethical approval: All analyses were based on previous published studies, thus no ethical approval are required.
Consent to participate: All analyses were based on previous published studies, thus no patient consent are required.
Consent to publish: All analyses were based on previous published studies, thus no consent to publish are required.
Authors contributions: The authors are grateful for the dedication of all the coinvestigators to the study. MJ Z and ZN Q searched electronic bibliographic databases, scored the quality of the articles, and discussed in disagreements, T W consulted if necessary. WJ Y and J Z collected and analyzed data. MJ Z wrote the full text. Wang Tao reviewed the full text.
Funding: The study was supported by Natural Science Basic Research Program of Shaanxi Province (Nos. 2022JM-587). But we declare that there is no conflict of interest.
Competing interests: The authors declare that they have no conflict of interest.
Availability of data and materials: We guaranteed the authenticity and validity of the data, and all the data comes from every document searched in the database.
References
- Sveinsson OA, Kjartansson O, Valdimarsson EM. Cerebral ischemia/infarction-diagnosis and treatment. Laeknabladid. 2014 Jul; 100(7-8): 393-401.
- Caprio FZ, Sorond FA. Cerebrovascular disease: Primary and secondary stroke prevention. Med Clin North Am. 2019; 103(2): 295-308.
- Novotny V, Khanevski AN, Bjerkreim AT, et al. Short-term outcome and in-hospital complications after acute cerebral infarcts in multiple arterial territories. Stroke. 2019; 50: 3625-3627.
- Benjamin EJ, Muntner P, Alonso A. et al. Heart Disease and Stroke Statistics—2019 Update: A Report From the American Heart. Circulation. 2019; 139(10): e56-e528.
- Mishra PJ, Banerjee D. Actvaton and Differentiation of Mesenchymal Stem Cells. Methods Mol Biol. 2017; 1554: 201-209.
- Catanese L, Tarsia J, Fisher M. Acute Ischemic Stroke Therapy Overview. CircRes. 2017; 120(3): 541-558.
- Smith EE, Saver JL, Cox M, et al. Increase in Endovascular Therapy in Get with the Guidelines-Stroke after the Publication of Pivotal Trials. Circulation. 2017; 136(24): 2303-2310.
- Lapchak PA, Araujo DM. Advances in hemorrhagic stroke therapy: Conventional and novel approaches. Expert Opin Emerg DR. 2007; 12(3): 389-406.
- Pittenger MF, Mackay AM, Beck SC, et al. Multilineage potential of adult human mesenchymal stem cells. Science. 1999; 284(5411): 143-147.
- Ren H, Sang Y, Zhang F, et al. Comparative analysis of human mesenchymal stem cells from umbilical cord, dental pulp, and menstrual blood as sources for cell therapy. Stem Cells Int. 2016; 2016: 3516574.
- Mitchell KE, Weiss ML, Mitchell BM, et al. Matrix cells from Wharton’s jelly form neurons and glia. Stem Cells. 2003; 21(1): 50–60.
- Le Blanc K, Tammik L, Sundberg B, et al. Mesenchymal stem cells inhibit and stimulate mixed lymphocyte cultures and mitogenic responses independently of the major histocompatibility complex. Scand J Immunol. 2003; 57(1): 11-20.
- Kim HJ, Park JS. Usage of human mesenchymal stem cells in cell-based therapy: advantages and disadvantages. Dev Reprod. 2017; 21(1): 1–10.
- Keating A. Mesenchymal stromal cells. Curr Opin Hematol. 2006; 13(6): 419–425.
- Shichinohe H, Kuroda S, Yano S, et al. Improved expression of gamma-aminobutyric acid receptor in mice with cerebral infarct and transplanted bone marrow stromal cells: an autoradiographic and histologic analysis. J Nucl Med. 2006; 47(3): 486–491.
- Bang OY, Lee JS, Lee PH, et al. Autologous mesenchymal stem cell transplantation in stroke patients. Ann Neurol. 2005; 57(6): 874-882.
- Lin YC, Ko TL, Shih YH, et al. Human umbilical mesenchymal stem cells promote recovery after ischemic stroke. Stroke. 2011; 42(7): 2045-2053.
- Hocum Stone LL, Xiao F, Rotschafer J, et al. Amelioration of ischemic brain injury in rats with human umbilical cord blood stem cells: mechanisms of action. Cell Transplant. 2016; 25 (8): 1473-1488.
- Shamseer L, Moher D, Clarke M, et al. PRISMA-P group: preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. 2015; 350: g7647.
- Cumpston M, Li T, Page MJ, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. Cochrane Database Syst Rev. 2019; 10(10): ED000142.
- Hooijmans CR, Rovers MM, de Vries RB, et al. SYRCLE’s risk of bias tool for animal studies. BMC Med Res Methodol. 2014; 26(14): 43.
- Zhengzheng Wu. Human umbilical cord mesenchymal stem cells protect ischemic stroke by regulating neuron-microglia crosstalk. Nanjing University. 2014.
- Yao Zhu. Human umbilical cord blood mesenchymal stem cells transplantation modulate inflammatory response and display neuroprotection at early stage in focal cerebral-reperfusion of rabbits. Anhui Medical University. 2014.
- Ying Zeng. Studies of Human Umbilical Cord Mesenchymal Stem Cells Intravenous Injective Transplantation via Vena Caudalis in Rats with Ischemic. Central South University. 2013.
- Xiaolan Chen, Renbin Huang, Yinjuan Tang, et al. Study on the therapeutic effects of the intravenous administration of human umbilical cord blood mesenchymal stem cells for treating focal cerebral ischemia in rats. Chinese Journal of Practical Neurological Diseases. 2007; 10(01): 4-7.
- Lei Du. Studies of Human Umbilical Cord Mesenchymal Stem Cells Transplantation in Rats with Ischemic. Hebei Medical University. 2008.
- Haili Huang, Yeming Guan, Xuechun Liu, et al. Effect of human umbilical cord blood mesenchymal stem cells transplantation on functional recovery and the1H-MRS parameters in the rabbits with cerebral ischemia-reperfusion. J Apoplexy and Nervous Diseases. 2017; 34(06): 484-487.
- Liping Shen, Shuaishuai Wang, Liguo Dong, et al. Intranasal administration of the conditioned medium of human umbilical cord-derived mesenchymal stem cells for treatment of cerebral ischemia-reperfusion injury. Chinese Journal of Tissue Engineering Research. 2013; 17(45): 7891-7897.
- Dicheng Zhao, Juan Du, Hong Chen, et al. Experimental Study on Treatment of Cerebral Ischemic Rats by Umbilical Cord Blood-Derived Mesenchymal Stem Cells. Chinese Journal of General Practice. 2012; 10(02): 172-173+182+333.
- Jingjing Zhou. Human umbilical cord blood mesenchymal stem cells transplantation improves inflammatory responses in ischemic stroke rats. Anhui Medical University. 2016.
- Pengdian Chen. Effects of electro-acupuncture at conception and governor vessels plus human umbilical cord blood-derived mesenchymal stem cells transplantation on nerve protection of cerebral ischemia rats. Guangzhou University of Chinese Medicine. 2014.
- Liang Hou, Fang Xu, Xuechun Liu, et al. Effect of human umbilical cord blood mesenchymal stem cells transplantation on Foxp3 expression in peripheral blood of errebral infarction rats. J Apoplexy and Nervous Diseases. 2016; 33(12): 1060-1063.
- Min Pi, Pengdian Chen, Zhuoxin Yang, et al. Effect of Governor Vessel Electro-acupuncture plus HUCB-MSCs Transplantation on Neurological Deficit Scores and Cellular Apoptosis of Cerebral Ischemia-Reperfusion Rats. Lishizhen Medicine and Materia Medica Research. 2014; 25(02): 492-495.
- Songhe Yin, Jun Chen, Li Ding, et al. Effect of Umbilical Cord Blood Mesenchymal Stem Cell Transplantationon Neural Function in Rats with Cerebral Infarction. Jinzhou Medical University. 2023 Apr; 44(02): 1-7.
- Meng Li, Chuanwen Li, Junqi Sun, et al. Effect of human umbilical cord blood mesenchymal stem cell transplantation on SIRT1-P53 pathway in rats with cerebral ischemia-reperfusion. Acta Universitatis Medicinalis Anhui. 2019; 54(04): 534-538.
- Zhai QY, Ren YQ, Ni QS, et al. Transplantation of Human Umbilical Cord Mesenchymal Stem Cells-Derived Neural Stem Cells Pretreated withNeuregulin1β Ameliorate Cerebral Ischemic Reperfusion Injury in Rats. Biomolecules. 2022; 12(3): 428.
- Chung DJ, Choi CB, Lee SH, et al. Intraarterially delivered human umbilical cord blood-derived mesenchymal stem cells in canine cerebral ischemia. J Neurosci Res. 2009; 87(16): 3554-2567.
- Nalamolu KR, Venkatesh I, Mohandass A, et al. Exosomes Treatment Mitigates Ischemic Brain Damage but Does NotImprove Post-Stroke Neurological Outcome. Cell Physiol Biochem. 2019; 52(6): 1280-1291.
- Zhao Q, Hu J, Xiang J, et al. Intranasal administration of human umbilical cord mesenchymal stem cells-conditioned medium enhances vascular remodeling after stroke. Brain Res. 2015; 1624: 489-496.
- Cheng Q, Zhang Z, Zhang S, et al. Human umbilical cord mesenchymal stem cells protect against ischemic brain injury in mouse by regulating peripheral immune inflammation. Brain Res. 2015; 1594: 293-304.
- Guan YM, Zhu Y, Liu XC, et al. Effect of human umbilical cord blood mesenchymal stem cell transplantation on neuronal metabolites in ischemic rabbits. BMC Neurosci. 2014; 15: 41.
- Park HW, Chang JW, Yang YS, et al. The Effect of Donor-Dependent Administration of Human Umbilical Cord Blood-Derived Mesenchymal Stem Cells following Focal Cerebral Ischemia in Rats. Exp Neurobiol. 2015; 24(4): 358-365.
- Mäkinen S, Kekarainen T, Nystedt J, et al. Human umbilical cord blood cells do not improves ensor imotor or cognitive outcome following transient middle cerebral artery occlusion in rats. Brain Res. 2006; 1123(1): 207-215.
- Lim JY, Jeong CH, Jun JA, et al. Therapeutic effects of human umbilical cord blood-derived mesenchymal stem cells after intrathecal administration by lumbar puncture in a rat model of cerebralischemia. Stem Cell Res Ther. 2011; 2(5): 38.
- Tsuji M, Taguchi A, Ohshima M, et al. Effects of intravenous administration of umbilical cord blood CD34(+) cells in a mouse model of neonatal stroke. Neuroscience. 2014; 263: 148-158.
- Park HW, Kim Y, Chang JW, et al. Effect of Single and Double Administration of Human Umbilical Cord Blood-Derived Mesenchymal Stem Cells Following Focal Cerebral Ischemia in Rats. ExpNeurobiol. 2017; 26(1): 55-65.
- Womble TA, Green S, Shahaduzzaman M, et al. Monocytes are essential for the neuroprotective effect of human cord blood cells following middle cerebral artery occlusion in rat. Mol Cell Neurosci. 2014; 59: 76-84.
- Ramdan M, Bigdeli MR, Khaksar S, et al. Evaluating the effect of transplanting umbilical cord matrix stem cells on ischemic tolerance in an animal model of stroke. Neurol Res. 2021; 43(3): 225-238.
- Bugos O, Bhide M, Zilka N. Beyond the rat models of human neurodegenerative disorders. Cell Mol Neurobiol. 2009; 29(6-7): 859-69.
- Z hang T, Lee YW, Rui YF, et al. Bone marrow-derived mesenchymal stem cells promote growth and angiogenesis of breast and prostate tumors. Stem Cell Res Ther. 2013; 4(3): 70.
- Huang L, Liu Y, Lu J, et al. Intraarterial transplantation of human umbilical cord blood mononuclear cells in hyperacute stroke improves vascular function. Stem Cell Res Ther. 2017; 8(1): 74.
- Shichita T, Ago T, Kamouchi M, et al. Novel therapeutic strategies targeting innate immune responses and early inflammation after stroke. J Neurochem. 2012; 123(Suppl 2): 29-38.
- Hayakawa K, Qiu J, Lo EH. Biphasic actions of HMGB1 signaling ininflammation and recovery after stroke. Ann N Y Acad Sci. 2010; 1207: 50-57.
- Cheng Q, Zhang Z, Zhang S, et al. Human umbilical cord mesenchymal stem cells protect against ischemic brain injury in mouse by regulating peripheral immune inflammation. Brain Res. 2015; 1594: 293-304.
- Zhu Y, Guan YM, Huang HL, et al. Human umbilical cord blood mesenchymal stem cell transplantation suppresses inflammatory responses and neuronal apoptosis during early stage of focal cerebral ischemia in rabbits. Acta Pharmacol Sin. 2014; 35(5): 585-591.
- Kurozumi K, Nakamura K, Tamiya T, et al. Mesenchymal stem cells that produce neurotrophic factors reduce ischemic damage in the rat middle cerebral artery occlusion model. MolTher. 2005; 11(1): 96-104.
- Gong Feng, Guoping Tian, Li Li, et al. Effect of human umbilical cord blood-derived mesenchymal stem cells in the treatment of cerebral infarction. Practical Journal of Cardioc Cerebral Pneumal and Vascular Diseases. 2014; 22(01): 28-30.
- Liping Tian, Jingjing Wang, Kailong Zhao. Clinical effect of human umbilical cord blood mesenchymal stem cells on cerebral infarction. Chinese Journal of Clinical Rational Drug Use. 2018; 11(26): 109-110.
- Yang WZ, Zhang Y, Wu F, et al. Safety evaluation of allogeneic umbilical cord blood mononuclear cell therapy for degenerative conditions. J Transl Med. 2010; 8: 75: 1-6.
- Boltze J, Schmidt UR, Reich DM, et al. Determination of the therapeutic time window for human umbilical cord blood mononuclear cell transplantation following experimental stroke in rats. Cell Transplant. 2012; 21(6): 1199-1211.