
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Research Article - Open Access, Volume 5
Artificial intelligence advances in cardiovascular imaging
Homayoon Yektaei; Arsalan Salari; Fatemeh Kazemi Lichaee*
Department of Cardiology, Heshmat Hospital, Cardiovascular Diseases Research Center, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran.
*Corresponding Author : Kazemi Lichaee F
Department of Cardiology, Cardiovascular Diseases Research Center, Heshmat Hospital, School of Medicine, Guilan University of Medical Sciences, Rasht, Iran.
Email: fkazemi566@gmail.com
ORCID ID: 0009-0009-4397-8600
Received : Mar 25, 2024
Accepted : Apr 09, 2024
Published : Apr 16, 2024
Archived : www.jcimcr.org
Copyright : © Kazemi Lichaee F (2024).
Abstract
The medical specialty of radiology has experienced several extremely important and influential technical developments in the past that have affected how medical imaging is deployed. Artificial Intelligence (AI) is potentially another such development that will introduce fundamental changes to the practice of radiology. Among the most promising clinical applications of AI is diagnostic imaging, and mounting attention is being directed at establishing and fine-tuning its performance to facilitate the detection and quantification of a wide array of clinical conditions. Case studies of computer-aided diagnosis have shown excellent accuracy and specificity for detecting small radiographic abnormalities with the potential to improve public health.
Advances in medical imaging and Artificial Intelligence (AI) have ushered in an era of possibilities in healthcare. The number of imaging studies is naturally increasing, and so there is a need to improve clinical throughput and loss detection. With the availability and use of large data sets, Artificial Intelligence (AI) has the potential to improve patient care at every stage of imaging. The current literature shows that in the long term, AI has shorter human error and time savings in clinical workflow through automatic segmentation of cardiac structures. In the future, artificial intelligence may extend the value of diagnosis based on images alone or a combination of images and clinical images, thus providing informed diagnosis, prognosis, and decision-making. This review aims to provide an in-depth examination of artificial intelligence in contemporary cardiac computed tomography, highlighting its dual significance in clinical practice and academic investigations.
Keywords: Artificial intelligence; Medical imaging; Computed tomography; Atherosclerosis; Risk prediction.
Citation: Yektaei H, Salari A, Kazemi Lichaee F. Artificial intelligence advances in cardiovascular imaging. J Clin Images Med Case Rep. 2024; 5(4): 2989.
Introduction
Artificial Intelligence (AI) is increasingly used to improve image interpretation and analysis in medical imaging. Artificial rhythms can be trained to analyze medical images, leading to more efficient diagnosis and treatment of various diseases. AI has revolutionized the way medical professionals diagnose and treat diseases with its volume of rapid and accurate analysis of huge amounts of data [1]. Artificial intelligence has revolutionized the way medical professionals diagnose and treat diseases by using it to quickly and accurately analyze massive amounts of data. Machine Learning (ML), on the other hand, is a subset of AI that specifically focuses on machines’ ability to learn from data, enhance their performance through experience, and make predictions. Artificial intelligence refers to the all-encompassing ability of mathematical algorithms to train machines to mimic human intelligence [2]. There are some AI and MI different applications in numerous industries [3,4]. Within the healthcare sector, there is a growing body of literature exploring ML-based algorithms and their potential clinical usefulness. With the use of programmed algorithms, machines can complete tasks, execute decisions, and recognize images. Machine learning is a branch of artificial intelligence that is particularly useful in the interpretation of therapeutic medical imaging, as information from various sources can be used for a doctor to perform tests. Machine learning can use a variety of different approaches to analyze a greater quantity of information. It can be classified as supervised or unsupervised. These two techniques are applied in different situations [5,6].
Modern cardiovascular diagnostics heavily rely on non-invasive imaging techniques, with cardiac Computed Tomography (CT) being recognized as a primary option for assessing cardiovascular risk and evaluating stable and unstable patients. Among the various diagnostic tests available, Coronary CT Angiography (CCTA) stands out with its exceptional sensitivity (95-99%) in detecting Coronary Artery Disease (CAD), defined as a stenosis of 50% or more on invasive coronary angiography. Its specificity ranges from 64% to 83%. The clinical advantages of using CCTA to diagnose stable CAD and guide subsequent decision-making have been demonstrated in two significant clinical trials: PROMISE (Prospective Multicenter Imaging Study for Evaluation of Chest Pain) and SCOT-HEART (Scottish Computed Tomography of the HEART). These trials, along with recent national and international guidelines, have solidified CCTA as a preferred first-line diagnostic test [7].
The field of modern medicine is marked by the production of a considerable volume of data, including advanced imaging techniques [8]. As the amount of medical information continues to grow rapidly, healthcare professionals are embracing innovative technologies to analyze these vast amounts of data efficiently, all while prioritizing patient safety and welfare. The emergence of Artificial Intelligence (AI) in the medical field has instilled optimism that it can enhance health outcomes by complementing human intelligence and optimizing the diagnostic and prognostic capabilities of current tests, thereby reducing the workload on physicians [9].
The aim of this review is to provide a comprehensive analysis of the applications of artificial imaging in cardiac CT, and its dual implications in clinical care and research and scientific discovery. Initially, we delve into the fundamental terms associated with AI such as ‘big data’, ‘Machine Learning’ (ML), ‘deep learning’, and ‘radionics’. Subsequently, we assess the current evidence, strengths, limitations, and prospects of AI in non-invasive cardiovascular imaging, utilizing cardiac CT as a prime example to highlight the numerous challenges and opportunities. Lastly, we propose a scientific framework to ensure the clinical and scientific validity of forthcoming studies in this innovative, yet immensely promising and captivating field.
Materials and methods
Echocardiography: Artificial intelligence can be successfully applied in echocardiography to address variance in image acquisition and interpretation. In addition, artificial and machine intelligence can help in the diagnosis and management of cardiac diseases. Determining Left Ventricular Ejection Fraction (LVEF) by Simpson’s rule (Biplane method of disk) can be obtained using artificial intelligence in this software. This automation makes the results more repeatable and independent of the operator, which means more quality and accuracy in diagnosis [10].
Cardiac magnetic resonance: AI is used for optimizing many aspects of CMR [11], including chamber quantification and ventricular function determination, perfusion and flow assessment, and tissue characterization. However, these algorithms are not fully automated, with an ongoing need for user input [12,14].
Enhanced accuracy and efficiency: In the future, AI may extend diagnostic value based on images alone or a combination of images and clinical images, thus providing informed diagnosis, prognosis, and decision-making [15,16]. Traditional methods of image interpretation often rely on human expertise, which can be subjective and prone to errors [17]. AI algorithms, on the other hand, can analyze medical images with incredible precision, detecting even the smallest abnormalities that might be missed by the human eye [18]. This not only leads to more accurate diagnoses but also enables early detection of diseases, potentially saving lives. There is also an opportunity to combine biomarker, genomics, proteomics, and metabolomics with imaging data to improve the predictive value of ML algorithms and create personalized healthcare for patients [19].
Myocardial Perfusion Imaging (MPI) with Electrocardiogram (ECG) SPECT is a useful imaging tool for diagnosing Coronary Artery Disease (CAD) and determining prognosis [20,23].
Artificial intelligence applications in cardiac and pacing imaging are growing. In the short term, the synthetic prosthesis has the potential to reduce human error and save time in the clinical workflow through automatic segmentation of cardiac structures [10,12].
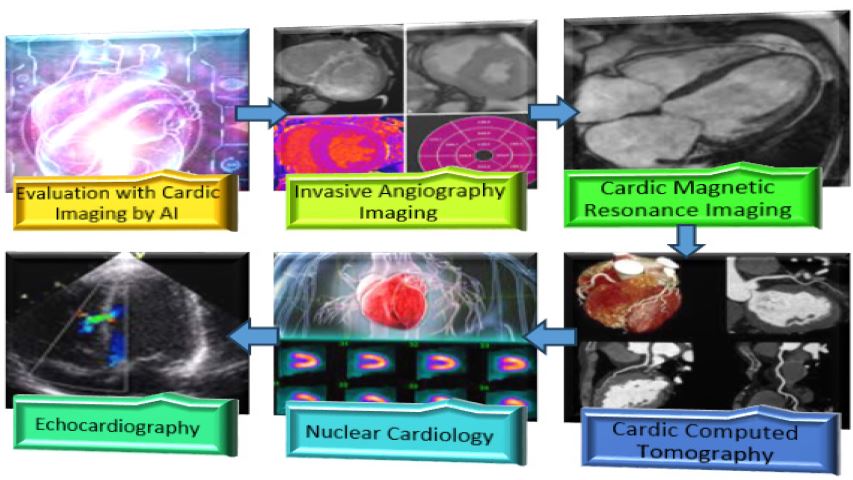
With the addition of machine learning to supplement the MPI results, patient-specific risk stratification is improved. A study by Głowacki et al. found evidence that machine learning is greater than parametric statistical models in predicting the presence of obstructive CAD, the need for revascularization, and potential adverse risks [24]. Specifically, Wang et al. conducted a study that evaluated the MPI device’s accuracy in predicting CAD and reversible perfusion deficit in training and validation cohorts. The results showed that Stress-only MPI with ML models can detect CAD [25]. Figure 1 shows Cardiac imaging modalities.
Cardiology and nuclear cardiometry use non-invasive techniques to measure blood flow in the heart [13]. This test is especially useful when diagnosing coronary disease and possible ischemia or checking the heart due to reduced blood use. Deep learning allows for a greater ability to analyze images by identifying high-dimensional patterns [14,15]. In this article, we review the advances of artificial intelligence’s effect on cardiovascular imaging and highlight its potential to improve outcomes.Figure 2 shows the effect of cardiovascular imaging by AI.
Enhanced accuracy and efficiency: One of the primary advantages of AI in medical imaging is its ability to enhance accuracy and efficiency in diagnosis. Traditional methods of image interpretation often rely on human expertise, which can be subjective and prone to errors. AI algorithms, on the other hand, can analyze medical images with incredible precision, detecting even the smallest abnormalities that might be missed by the human eye. This not only leads to more accurate diagnoses but also enables early detection of diseases, potentially saving lives [21,22].
By leveraging machine learning algorithms, AI systems can analyze medical images with speed and precision, aiding in the identification of early-stage diseases that may be difficult to detect through traditional methods [23]. This early detection is crucial as it can lead to timely interventions, potentially saving lives and improving treatment outcomes [24].
One of the key advantages of AI in medical imaging is its ability to enhance the accuracy and efficiency of disease diagnosis [25].
Improved treatment planning: AI in medical imaging goes beyond diagnosis; it also plays a crucial role in treatment planning. By analyzing medical images, AI algorithms can provide valuable insights into disease progression, tumor growth, and response to treatment [27]. This information helps healthcare professionals develop personalized treatment plans, optimizing patient care and outcomes [28,29]. Additionally, AI can assist in surgical planning by providing 3D reconstructions and virtual simulations, allowing surgeons to visualize and prepare for complex procedures [30].
Enhanced screening and early detection: Screening for diseases like cancer often involves analyzing a large number of imimages, which can be time-consuming and resource-intensive. AI algorithms excel in this area by quickly and accurately analyzing vast amounts of data, enabling efficient screening processes. By detecting early signs of diseases, AI can significantly improve the chances of successful treatment and reduce healthcare costs associated with advanced-stage diagnoses [31].
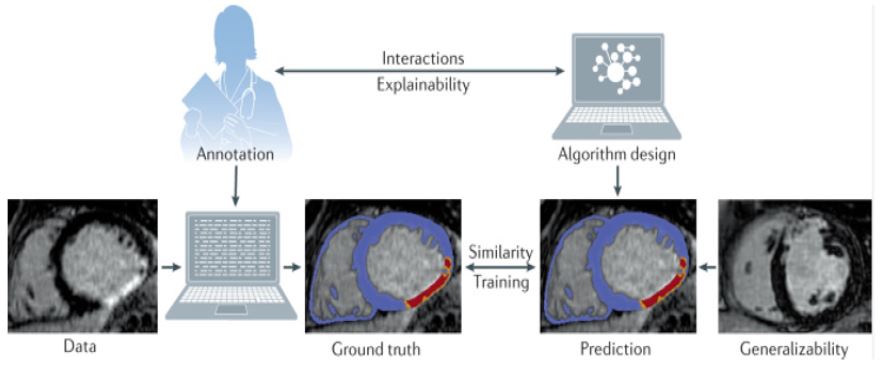
For image segmentation or detection tasks, large numbers of experts must create training and validation data by labeling the images and annotating the structures of interest [32]. Research is needed on newer tools that reduce the annotation burden on human experts. For example, some algorithms can semiautomatically trace structures on images, so that a human annotator need only modify machine-generated traces, rather than generate each annotation de novo [33,34]. It is possible to train deep learning methods in a semi supervised manner with minimally annotated data sets to get reasonable approximations of structures, thereby iteratively reducing the human effort in tracing structures [35,36].
Deep learning uses multiple layers to progressively extract higher level features from raw image input [37]. It helps to disentangle the abstractions and picks out the features that can improve performance. The concept of deep learning was proposed decades ago [38]. Only till recent decade, the application of deep learning became feasible due to enormous number of medical images being produced and advancements in the development of hardware.
Use of machine learning for efficient image annotation: For image segmentation or detection tasks, large numbers of experts must create training and validation data by labeling the images and annotating the structures of interest. Research is needed on newer tools that reduce the annotation burden on human experts. For example, some algorithms can semiautomatically trace structures on images, so that a human annotator need only modify machine-generated traces, rather than generate each annotation de novo [38]. It is possible to train deep learning methods in a semi supervised manner with minimally annotated data sets to get reasonable approximations of structures, thereby iteratively reducing the human effort in tracing structures [28].
Challenges and future directions: While AI in medical imaging holds immense promise, it also faces certain challenges [39]. Data privacy, regulatory compliance, and ethical considerations are crucial aspects that need to be addressed to ensure the responsible and secure use of AI in healthcare. Additionally, ongoing research and development are necessary to refine AI algorithms, improve interpretability, and validate their performance across diverse patient populations [28].
Cardiac magnetic resonance: AI is used for optimizing many aspects of CMR, including chamber quantification and ventricular function determination, perfusion and flow assessment and tissue characterization. However, these algorithms are not fully automated, with an ongoing need for user input [31].
Novel AI applications in CMR: Magnetic Resonance Fingerprinting (MRF) is a new technique that allows the quantificaquantification of multiple tissue properties in a single scan. A recent study investigated the use of cardiac MRF (cMRF) for myocardial T1, T2 and Extracellular Volume (ECV) quantification in 9 patients with non-ischemic cardiomyopathy compared with traditional mapping methods [40]. Due to the potential of cMRF to overcome variations in heart rate s and system properties, cMRF may achieve more reproducible T1 and T2 quantification, and therefore holds promise for application in cardiomyopathy patients [41].
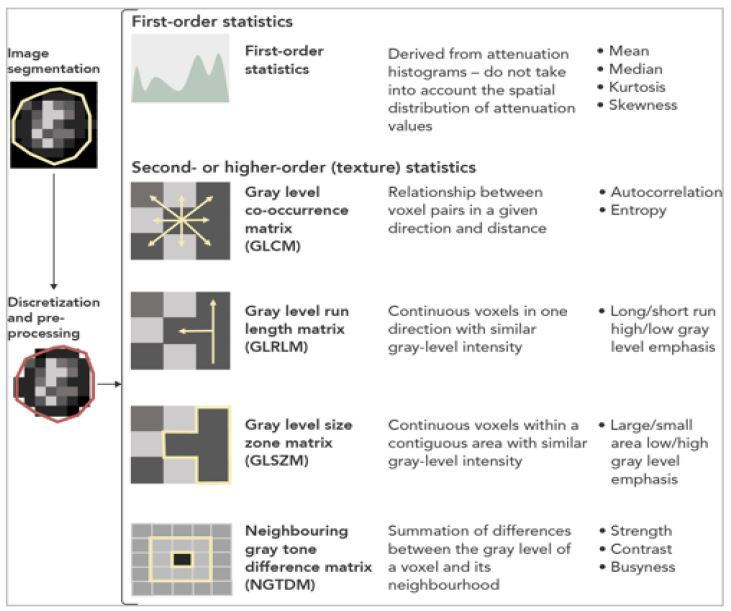
Radiomics: A link between CT imaging and machine learning: Radiomics is the utilization of intricate mathematical formulas on a specific radiological image, such as a CT scan, to derive a multitude of characteristics [42]. These characteristics pertain to the shape, attenuation, and texture of a particular volume of interest [43]. Figure 3 illustrates this concept. Being an isotropic imaging technique comprised of overlaid numerical matrices, specifically Hounsfield Unit (HU) values, CT scans are highly suitable for the implementation of radiomic approaches [44].
Machine learning and radiomics in cardiovascular medicine from electrocardiogram to cardiac CT: To date, AI methods in the field of Cardiology have primarily concentrated on the interpretation of Electrocardiogram (ECG) and echocardiogram results, Utilizing Deep Neural Networks (DNNs). These tests have provided researchers with a wealth of data to train their algorithms [46]. DNNs have exhibited a high level of accuracy in diagnosing acute myocardial infarction (approximately 93% sensitivity and 90% specificity), as well as classifying arrhythmias and electrical conduction abnormalities, comparable to the accuracy of trained cardiologists [47]. A recent groundbreak ing study showcased the power of big data and AI by analyzing a large cohort of 180,922 patients with 649,931 normal sinus rhythm ECGs. The study demonstrated that a CNN algorithm could reliably detect the presence of atrial fibrillation, with an Area Under the Curve (AUC) of 0.87 (95% confidence interval 0.86-0.88). However, as cardiac CT scans have become increasingly popular for non-invasive assessment of Coronary Artery Disease (CAD), the focus of AI research has expanded to include the analysis and interpretation of these scans [45].
Table 1: Supervised and unsupervised approaches to machine learning.
| Supervised | |
|---|---|
| Regression analysis [48,49] | Uncomplicated form of supervised machine learning that generates an algorithm to describe a relationship between multiple variables and an outcome of interest. Stepwise models “automatically” add or remove variables based on the strength of their association with the outcome variable, until a significant model is developed or“learned.” |
| Support vector machines [50,51] | While regression analysis may identify linear associations, "support vector machines" provide non-linear models by defining "planes" at the highest point that best assign features to groups that produce certain outcomes. They provide, gives. They predict, distinguish. |
| Random forests [52] | Identify the best cut point values in different features of individual groups of related data to be able to separate them out to predict a particular outcome. |
| Neural networks [53] | The features are fed through a node network of decision points, which is meant to mimic human brain processing. |
| Convoluted neural networks [54] | A multilayered network, often applied to image processing, simulating some of the properties of the human visual cortex. A mathematical model is used to transfer the results to successive layers. |
| Deep Learning (DL) [55] | DL is defined as a class of neural network algorithms where more internal layers are used than traditional neural networks ("deep" simply describes a layer separation). The title is described as Convolutional Neural Networks. |
| Unsupervised | |
| Principal component analysis [56] | Simple form of unsupervised learning in which the features that account for the most variation in a dataset can be identified. |
| Hierarchical clustering [55,56] | It creates a hierarchical decomposition of the data based on similarity with another cluster by aggregating them (an agglomerative approach) or dividing them as it moves down in hierarchy (a divisive approach). Strengths - Easy to understand and visualize using dendrograms, insensitive to outliers. Answer - metric measures and arbitrary linkage do not work with missing data, may lead to misinterpretation of dendrogram, difficulty in finding optimal solution. |
| Partitioning algorithms [57] | A form of cluster analysis that determines the degree of separation of different features in a data set and tries to find groups in which features are most differentiated. It does this by defining similarity based on proximity to the center of the cluster. The algorithm modulates the data to build clusters with repeated value of the distance from the center. Strengths - Simple and easy to implement, easy to interpret, fast and efficient. Despite being performed and interpreted, it is at heart and relatively unused. Variables - uniform cluster size, may weaken with different cluster densities, sensitive to outliers. |
| Model-based clustering [58] | This clustering algorithm makes a general assumption that each cluster generates a probabilistic (mostly Gaussian) model. Strengths - a description for the components, which is possible to evaluate clusters within clusters, number of clusters. Computationally intensive problems may converge slowly. |
| Grid-based algorithms [59] | Strengths—can work on large multidimensional space, reduction in computational complexity, data space partitioned to finite cells to form grid structure. Difficulties—difficult to handle irregular data distributions; limited by predefined cell sizes, borders, and density threshold; difficult to cluster high-dimensional data. |
| Density-based spatial clustering of applications with noise [60] | Strengths - does not require cluster counts, can find arbitrary problems that are robust to outliers. Decisions - not definitive, quality varies by size, cannot tolerate large differences in density. |
Coronary plaque phenotyping: While the identification of coronary plaques and their hemodynamic importance depends on a machine learning approach that combines various metrics derived from CCTA, a more thorough evaluation of the plaque microenvironment, histology, and overall biology necessitates a more detailed radiomic analysis of its phenotype [61].
These high-risk plaque characteristics provide personalized insights into the vascular biology of each plaque. For example, the remodeling of the vascular wall in atherosclerosis is the result of complex pathways that lead to cell migration and remodeling of the extracellular matrix. This is often caused by an imbalance in the expression and activity of matrix metalloproteinases and their inhibitors in the plaque’s microenvironment [62]. The resulting outward remodeling of the blood vessels can be detected on CCTA as an increase in vascular diameter around the plaque, which is captured by the remodeling index. On the other hand, low-attenuation plaque is associated with a lipid-rich necrotic core, which is an extracellular mass in the intima caused by the necrosis and apoptosis of lipid-laden macrophage foam cells. This high-risk plaque phenotype, characterized by a thin fibrotic cap above a necrotic core, is often referred to as a ‘Napkin-Ring Sign’ (NRS) on CCTA [63]. It appears as a low-attenuation area surrounded by a high-attenuation rim. Lastly, spotty calcification indicates inflamed areas of continuous coronary calcification and microcalcification. Vascular calcification is a localized response to an inflammatory microenvironment, with a clear connection between the infiltration of inflammatory cells and osteoblastic metaplasia [64].
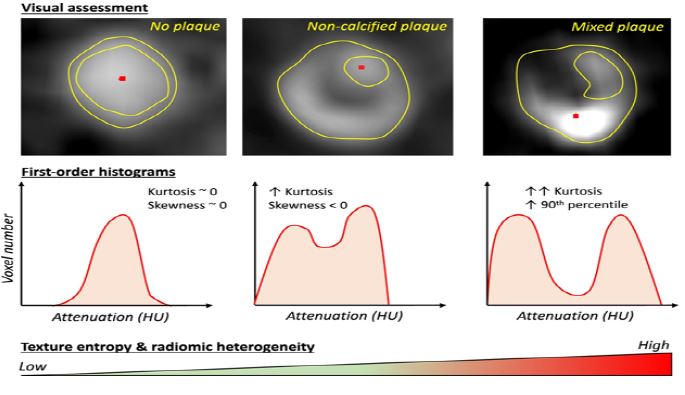
Radiomic phenotyping of a specific plaque has the potential to identify high-risk plaque characteristics, such as changes in the attenuation histogram and radiomic texture. This approach aims to standardize a process that is often subjective and dependent on the operator. In a study conducted by Kolossvary et al., 30 non-ruptured plaque lesions (NRS) and 30 non-NRS plaques with similar levels of calcification, luminal obstruction, localization, and imaging parameters were analyzed. The results showed that 916 radiomic features were significantly different between the two groups, with 418 of these features achieving an Area Under the Curve (AUC) of greater than 0.80. Notably, texture-shape statistics, such as short- and long-run low grey-level emphasis, exhibited the highest AUC values of 0.918 and 0.894, respectively. In contrast, none of the conventional metrics derived from Coronary Computed Tomography Angiography (CCTA) were able to discriminate between the two groups [65].
Furthermore, a more recent analysis involving 44 plaques from 25 patients who underwent multimodality imaging demonstrated that radiomic parameters derived from CCTA outperformed conventional metrics in identifying specific plaque characteristics. These included intravascular ultrasound-defined attenuated plaques, optical coherence tomography-detected thin-cap fibroatheroma, and 18F-sodium fluoride (18F-NaF) positivity on Positron Emission Tomography (PET), which serves as a marker for microcalcification and coronary inflammation.
Lastly, in an ex vivo analysis of 445 cross-sections taken from 21 coronary arteries of seven male hearts, a radiomics-based machine learning model was found to be superior to visual assessment, low attenuation, and mean Hounsfield Units (HU) in identifying advanced atheromatous lesions. Finally, in an analysis of 445 cross-sections taken from 21 coronary arteries from seven male hearts imaged in vitro, a radiomics-based ML model was found to be superior to visual evaluation (AUC=0.73 vs. 0.65; P=0.04), low attenuation (AUC=0.55; P=0.01), and mean HU (AUC=0.53; P=0.004) in the identification of advanced atheromatous lesions [66,67]. Coronary lesions can be phenotypically characterized through radiomics. Variations in the composition of coronary bridges are reflected in distinct radiomic tissue patterns observed during computed tomography analysis. These patterns can be quantified using first and higher order radiomic features. By analyzing and analyzing changes in these features, an automated feature can not only identify plaque, but also provide a comprehensive understanding of the histology and biology associated with a specific lesion [66]. Figure 6 shows the process.
AI methods in cardiovascular imaging: Two distinct applications of artificial intelligence in cardiac imaging have been reported. Classical ML methods have been used with many clinical image features and/or predicted predictions to distinguish outcomes or prognoses from large datasets. More advanced AI methods, such as DL methods, are used on real images for manual recognition [68]. Conventional AI methods, DL, do not require engineering (i.e., computation and customized imaging transformation features), but instead directly interrogate images for image segmentation or outcome prediction tasks. DL is particularly well-suited for large and highly characterized datasets – for example, genomic and imaging datasets [69].
Similar to the way humans learn, AI algorithms need training examples to perform a task confidently. This is a more general formalization of artificial intelligence, which defines intelligent algorithms as algorithms that increase their performance on a specific task as they gain experience [70] (Figure 5).
Fully automated diagnosis: While most of the current applications of ML are on cardiac imaging surfaces and image segmentation or some of the methods are used, there are also researches and disease classification and diagnosis based on ML. Ultimately, the physician’s final clinical diagnosis usually requires considering additional clinical in-formation such as age, patient history [71].
ML methods can potentially provide a rapid and precise computation of post-imaging disease or outcome probability, based on the integration of imaging and clinical variables. This approach was demonstrated in several recent studies, particularly in SPECT MPI, where the level of automation for image analysis is high compared to other modalities [72]. The AUC for revascularization prediction by ML was similar to that for the visual scores of one reader and superior to that of the other reader (Figure 6) [66,68].
Discussion
In the current era of advancing digitalization and the accumulation of extensive medical data and images, Artificial Intelligence (AI) and Machine Learning (ML) present innovative solutions to long-standing challenges in disease diagnosis and risk prediction. Simultaneous progress in the field of radiomics now allows mapping from CT scans of normal hearts, and many features can be developed that can introduce ML algorithms to increase the accuracy of heart disease diagnosis and risk assessment. These breakthroughs have the potential to revolutionize the landscape of healthcare by relieving clinicians of image processing and diagnostic and prognostic measurements. This, in turn, can lead to significant clinical and health economic advantages. Although still in its early stages, AI-based cardiovascular imaging holds great promise for both patients and healthcare providers, as it facilitates the transition towards a more personalized model of care. Computed tomography radiomics has emerged as a promising approach in precision medicine. In this proposed workflow, machine learning-powered radiomic analysis of cardiac computed tomography scans is integrated into clinical practice. By leveraging radiomic analysis, the time required for analysis can be significantly reduced. Furthermore, when combined with electronic health records, automated recommendations can be generated for physicians, aiding in diagnosis and patient prognosis. This integration of artificial and human intelligence allows physicians to make informed decisions and select the most suitable management plan based on comprehensive data.
Results
Overview of select ML algorithms: There exist 2 primary categories of machine learning algorithms, as illustrated in Table 2. The first category is supervised learning, which pertains to scenarios where both inputs and known outputs are available. The primary objective of these algorithms is to accurately establish a mapping between the inputs and outputs. Within supervised learning, regression algorithms are employed when dealing with continuous outputs, while classification algorithms are utilized for non-continuous or categorical outputs. On the other hand, unsupervised learning involves situations where labeled outputs are absent. The main purpose of unsupervised learning algorithms is to uncover and comprehend the underlying structure of the data itself.
The use of artificial intelligence in cardiac imaging and study has increased [80,98,99]. Brown et al. did research on using of artificial intelligence for rheumatic heart disease detection by Echocardiography. They concluded that artificial intelligence has the potential to detect RHD as accurately as expert cardiologists and to improve with more data [81]. Föllmer et al. have investigated the use of artificial intelligence for imaging of vulnerable atherosclerotic plaque in coronary arteries. They have reviewed the available evidence on the use of Artificial Intelligence in non-invasive and invasive coronary imaging [82].
Table 2: Examples of machine learning algorithms.
| Algorithm | Type | Basic description |
|---|---|---|
| K-means clustering [68] | Unsupervised | A set of k centroids is generated to establish clusters of data, with each data point being assigned to the centroid that is closest to it. |
| Hierarchical clustering [73] | Unsupervised | A hierarchical structure of clusters is constructed by merging the clusters that are closest to each other. Subsequently, the distances between the clusters are recalculated, leading to the eventual creation of a tree or dendrogram representing the clusters. |
| Principal component analysis [74] | Unsupervised | Principal Component Analysis (PCA) is a technique used for dimensionality reduction, which aims to enhance data compressibility by reducing the number of data points or dimensions. The primary objective of PCA is to simplify the complexity of the data while preserving its underlying structure. |
| Singular value decomposition [75] | Unsupervised | A framework that enables the decomposition of a large data matrix into a multiplication of smaller matrices. |
| Naïve Bayes theorem [76] | Supervised | The assumption of independence among predictors is made by a straightforward and effective algorithm. |
| K-nearest neighbors [77] | Supervised | All existing cases are stored and new cases are allocated based on a similarity metric. |
| Support vector machine [78] | Supervised | A new instance classifier that is characterized by a dividing hyperplane that classifies novel samples. |
| Random forest [76] | Supervised | The ensemble is comprised of numerous decision trees, functioning collectively. Each tree offers a class prediction, and the prediction that receives the highest number of votes is considered as the final prediction of the overall model. |
| Extreme gradient boosting [79] | Supervised | An ensemble technique is employed to construct a robust model by utilizing multiple weaker models, which are represented as short decision trees. To predict the residual values between the actual values and the robust model, a novel weak model is generated. These weak models are subsequently incorporated into the overall robust model in an iterative manner. |
| Decision tree [79] | Supervised | The tree will divide into branches or edges based on certain conditions or internal nodes. The branches that do not further divide are the decisions or leaves of the tree, which indicate the predicted outcome. Recursive binary splitting is a technique used to determine how the data is divided, and it relies on a cost function to identify the splits that result in the least accuracy loss for the model. |
| Auto MAPSE [80] | Supervised | AutoMAPSE was more precise than manual measurements if it averaged more heartbeats. AutoMAPSE had acceptable trending ability (concordance rate 81%) during hemodynamic alterations. In conclusion, autoMAPSE is feasible as an automatic tool for rapid and quantitative assessment of LV function, indicating its potential for hemodynamic monitoring. |
| SVM‐based method [81] | Supervised | Artificial intelligence has the potential to detect RHD as accurately as expert cardiologists and to improve with more data. These innovative approaches hold promise to scale echocardiography screening for RHD. |

Conclusion
Artificial intelligence has transformed the field of medical imaging, offering unprecedented accuracy, efficiency, and insights. From improving diagnosis and treatment planning to enhancing screening and early detection, AI has the potential to revolutionize healthcare. As technology continues to advance, it is crucial for healthcare professionals, policymakers, and researchers to collaborate and harness the power of AI to improve patient outcomes and shape the future of medical imaging.
There has been a rapid recent increase in the application of AI, ML and DL approaches in multimodality CVI. While AI and EHRs may hold the promise to bring a personalized approach to treatment of CV conditions in the future, the current practicing cardiologists need to be fully aware of the strengths and limitations of the current applications of AI. More multi-center studies are required to demonstrate that AI-based approaches are indeed superior to current conventional diagnostic and treatment pathways. More multi -center data are also required to increase the generalizability and applicability of these approaches.
Although there is an expanding body of literature on AI and ML in cardiovascular medicine, the future these fields will have in clinical practice remains to be paved. In particular, there is a promising role in providing automated imaging interpretation, automated data extraction and quality control, and clinical risk prediction, although these techniques require further refinement and evaluation.
Declarations
Declaration of interests: The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Consent to participate: Prior to study inclusion, written informed consent was given by all participants.
Authors contributions statement: H.Y: Writing – original draft, Methodology, Investigation. A.S Review & editing, Methodology. F.K: Writing – review & editing, Investigation, Supervision.
References
- Alanazi MR. The Future Evolution of Artificial Intelligence in Healthcare: A Comprehensive Analysis. 2024.
- Begum S, DebRoy S. Current Progress and Future Prospects of Artificial Intelligence in Education: A.
- Sikka MP, Sarkar A, Garg S. Artificial intelligence (AI) in textile industry operational modernization. Research Journal of Textile and Apparel. 2024; 28(1): 67-83.
- AL-Dosari K, Fetais N, Kucukvar M. Artificial intelligence and cyber defense system for banking industry: A qualitative study of AI applications and challenges. Cybernetics and systems. 2024; 55(2): 302-30.
- Guersenzvaig A. Can machine learning make naturalism about health truly naturalistic? A reflection on a data-driven concept of health. Ethics and Information Technology. 2024; 26(1): 2.
- Bardos A, Doupidis P, Kotsiopoulos T, Vafeiadis T, Nizamis A, Geerdens H, et al. Anomaly Detection in Industrial Processes: Supervised vs. Unsupervised Learning and the Role of Explainability. Unsupervised Learning and the Role of Explainability.
- Wong KK, Fortino G, Abbott D. Deep learning-based cardiovascular image diagnosis: a promising challenge. Future Generation Computer Systems. 2020; 110: 802-11.
- Oikonomou EK, Siddique M, Antoniades C. Artificial intelligence in medical imaging: a radiomic guide to precision phenotyping of cardiovascular disease. Cardiovascular Research. 2020; 116(13): 2040-54.
- Knuuti J, Wijns W, Saraste A, Capodanno D, Barbato E, Funck-Brentano C, et al. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes: the Task Force for the diagnosis and management of chronic coronary syndromes of the European Society of Cardiology (ESC). European heart journal. 2020; 41(3): 407-77.
- Crespin E, Rosier A, Ibnouhsein I, Gozlan A, Lazarus A, Laurent G, et al. Improved diagnostic performance of insertable cardiac monitors by an artificial intelligence-based algorithm. Europace. 2024; 26(1): 375.
- Kouzehkonan VG, Finn JP. Artificial intelligence in cardiac MRI. Intelligence-Based Cardiology and Cardiac Surgery: Elsevier. 2024; 191-9.
- Tandon A. Artificial intelligence in pediatric and congenital cardiac magnetic resonance imaging. Intelligence-Based Cardiology and Cardiac Surgery: Elsevier. 2024; 201-9.
- Sveric KM, Ulbrich S, Dindane Z, Winkler A, Botan R, Mierke J, et al. Improved assessment of left ventricular ejection fraction using artificial intelligence in echocardiography: A comparative analysis with cardiac magnetic resonance imaging. International Journal of Cardiology. 2024; 394: 131383.
- Hanneman K, Playford D, Dey D, van Assen M, Mastrodicasa D, Cook TS, et al. Value creation through artificial intelligence and cardiovascular imaging: a scientific statement from the American Heart Association. Circulation. 2024; 149(6): 296-e311.
- Karalis VD. The Integration of Artificial Intelligence into Clinical Practice. Applied Biosciences. 2024; 3(1): 14-44.
- Fan W, Liu H, Zhang Y, Chen X, Huang M, Xu B. Diagnostic value of artificial intelligence based on computed tomography (CT) density in benign and malignant pulmonary nodules: a retrospective investigation. PeerJ. 2024; 12: 16577.
- Egemen D, Perkins RB, Cheung LC, Befano B, Rodriguez AC, Desai K, et al. Artificial intelligence–based image analysis in clinical testing: lessons from cervical cancer screening. JNCI: Journal of the National Cancer Institute. 2024; 116(1): 26-33.
- Sherani AMK, Khan M, Qayyum MU, Hussain HK. Synergizing AI and Healthcare: Pioneering Advances in Cancer Medicine for Personalized Treatment. International Journal of Multidisciplinary Sciences and Arts. 2024; 3(01): 270-7.
- Ogunjobi TT, Ohaeri PN, Akintola OT, Atanda DO, Orji FP, Adebayo JO, et al. Bioinformatics Applications in Chronic Diseases: A Comprehensive Review of Genomic, Transcriptomics, Proteomic, Metabolomics, and Machine Learning Approaches. Medinformatics. 2024.
- Rozanski A, Miller RJ, Han D, Gransar H, Hayes SW, Friedman JD, et al. Comparative predictors of mortality among patients referred for stress SPECT versus PET myocardial perfusion imaging. Journal of Nuclear Cardiology. 2024: 101811.
- Wang J, Chen Y, Chu H, Pang Z, Hsu B, Li J. Feasibility of Myocardial Blood Flow Quantification to Detect Flow-limited coronary artery disease with A One-day Rest/Stress Continuous Rapid Imaging Protocol on Cardiac-dedicated CZT SPECT. Journal of Nuclear Cardiology. 2024: 101825.
- Rammos A, Bechlioulis A, Kekiopoulou A, Kekiopoulos P, Katsouras CS, Sioka C. Myocardial Perfusion Imaging and C-Reactive Protein in Myocardial Ischemia: A Retrospective Single-Center Study. Life. 2024; 14(2): 261.
- Zhao Y, Hu Y, Li Y, Wang Y, Xiao Y, Xu L, et al. Spherization indices measured by resting SPECT improve risk stratification in patients with ischemia with non-obstructive coronary artery disease (INOCA). EJNMMI research. 2024; 14(1): 1-10.
- Głowacki J, Krysiński M, Czaja-Ziółkowska M, Wasilewski J. Machine learning-based algorithm enables the exclusion of obstructive coronary artery disease in the patients who underwent coronary artery calcium scoring. Academic Radiology. 2020; 27(10): 1416-21.
- Wang F, Yuan H, Lv J, Han X, Zhou Z, Lu W, et al. Stress-only versus rest-stress SPECT MPI in the detection and diagnosis of myocardial ischemia and infarction by machine learning. Nuclear Medicine Communications. 2024; 45(1): 35-44.
- Sermesant M, Delingette H, Cochet H, Jais P, Ayache N. Applications of artificial intelligence in cardiovascular imaging. Nature Reviews Cardiology. 2021; 18(8): 600-9.
- Wang C, Zhu X, Hong JC, Zheng D. Artificial intelligence in radiotherapy treatment planning: present and future. Technology in cancer research & treatment. 2019; 18: 1533033819873922.
- Panayides AS, Amini A, Filipovic ND, Sharma A, Tsaftaris SA, Young A, et al. AI in medical imaging informatics: current challenges and future directions. IEEE journal of biomedical and health informatics. 2020; 24(7): 1837-57.
- Lewis SJ, Gandomkar Z, Brennan PC. Artificial Intelligence in medical imaging practice: looking to the future. Journal of Medical radiation sciences. 2019; 66(4): 292-5.
- Park JJ, Tiefenbach J, Demetriades AK. The role of artificial intelligence in surgical simulation. Frontiers in Medical Technology. 2022; 4: 1076755.
- Tippareddy C, Zhao W, Sunshine JL, Griswold M, Ma D, Badve C. Magnetic resonance fingerprinting: an overview. European Journal of Nuclear Medicine and Molecular Imaging. 2021;48(13):4189-200.
- Tajbakhsh N, Jeyaseelan L, Li Q, Chiang JN, Wu Z, Ding X. Embracing imperfect datasets: A review of deep learning solutions for medical image segmentation. Medical Image Analysis. 2020; 63: 101693.
- Meijering E, Jacob M, Sarria JC, Steiner P, Hirling H, Unser eM. Design and validation of a tool for neurite tracing and analysis in fluorescence microscopy images. Cytometry Part A: the journal of the International Society for Analytical Cytology. 2004; 58(2): 167-76.
- Hoogi A, Beaulieu CF, Cunha GM, Heba E, Sirlin CB, Napel S, et al. Adaptive local window for level set segmentation of CT and MRI liver lesions. Medical image analysis. 2017; 37: 46-55.
- Ouali Y, Hudelot C, Tami M. An overview of deep semi-supervised learning. arXiv preprint arXiv:200605278. 2020.
- LeCun Y, Bengio Y, Hinton G. Deep learning. nature. 2015; 521(7553): 436-44.
- Zhang Y, Chen J, Ma X, Wang G, Bhatti UA, Huang M. Interactive medical image annotation using improved Attention U-net with compound geodesic distance. Expert Systems with Applications. 2024; 237: 121282.
- Weston AD, Korfiatis P, Kline TL, Philbrick KA, Kostandy P, Sakinis T, et al. Automated abdominal segmentation of CT scans for body composition analysis using deep learning. Radiology. 2019; 290(3): 669-79.
- Younis HA, Eisa TAE, Nasser M, Sahib TM, Noor AA, Alyasiri OM, et al. A Systematic Review and Meta-Analysis of Artificial Intelligence Tools in Medicine and Healthcare: Applications, Considerations, Limitations, Motivation and Challenges. Diagnostics. 2024; 14(1): 109.
- Cherezov D, Viswanathan VS, Fu P, Gupta A, Madabhushi A. Rank acquisition impact on radiomics estimation (AсquIRE) in chest CT imaging: A retrospective multi-site, multi-use-case study. Computer Methods and Programs in Biomedicine. 2024; 244: 107990.
- Gillies RJ, Kinahan PE, Hricak H. Radiomics: images are more than pictures, they are data. Radiology. 2016; 278(2): 563-77.
- Hell MM, Achenbach S. CT support of cardiac structural interventions. The British Journal of Radiology. 2019; 92(1098): 20180707.
- Kolossváry M, Kellermayer M, Merkely B, Maurovich-Horvat P. Cardiac computed tomography radiomics. Journal of thoracic imaging. 2018; 33(1): 26-34.
- Sutanto H. Transforming Clinical Cardiology Through Neural Networks and Deep Learning: A Guide for Clinicians. Current Problems in Cardiology. 2024: 102454.
- Hannun AY, Rajpurkar P, Haghpanahi M, Tison GH, Bourn C, Turakhia MP, et al. Cardiologist-level arrhythmia detection and classification in ambulatory electrocardiograms using a deep neural network. Nature medicine. 2019; 25(1): 65-9.
- Attia ZI, Noseworthy PA, Lopez-Jimenez F, Asirvatham SJ, Deshmukh AJ, Gersh BJ, et al. An artificial intelligence-enabled ECG algorithm for the identification of patients with atrial fibrillation during sinus rhythm: a retrospective analysis of outcome prediction. The Lancet. 2019; 394(10201): 861-7.
- Mayr A, Binder H, Gefeller O, Schmid M. The evolution of boosting algorithms. Methods of information in medicine. 2014; 53(06): 419-27.
- Lin A, Kolossváry M, Išgum I, Maurovich-Horvat P, Slomka PJ, Dey D. Artificial intelligence: improving the efficiency of cardiovascular imaging. Expert review of medical devices. 2020; 17(6): 565-77.
- Gudigar A, Kadri NA, Raghavendra U, Samanth J, Inamdar MA, Prabhu MA, et al. Directional-Guided Motion Sensitive Descriptor for Automated Detection of Hypertension Using Ultrasound Images. IEEE Access. 2024.
- Saha P, Marouf Y, Pozzebon H, Guergachi A, Keshavjee K, Noaeen M, et al. Predicting time to diabetes diagnosis using random survival forests. medRxiv. 2024; 2024.02: 03.24302304.
- Bober-Irizar M, Banerjee S. Neural networks for abstraction and reasoning: Towards broad generalization in machines. arXiv preprint arXiv:240203507. 2024.
- Zeman AA, Ritchie JB, Bracci S, Op de Beeck H. Orthogonal representations of object shape and category in deep convolutional neural networks and human visual cortex. Scientific reports. 2020;10(1): 2453.
- Lundervold AS, Lundervold A. An overview of deep learning in medical imaging focusing on MRI. Zeitschrift für Medizinische Physik. 2019; 29(2): 102-27.
- Alloghani M, Al-Jumeily D, Mustafina J, Hussain A, Aljaaf AJ. A systematic review on supervised and unsupervised machine learning algorithms for data science. Supervised and unsupervised learning for data science. 2020: 3-21.
- Gupta A, Sharma H, Akhtar A. A comparative analysis of k-means and hierarchical clustering. EPRA International Journal of Multidisciplinary Research (IJMR). 2021; 7(8).
- Giordani P, Ferraro MB, Martella F, Giordani P, Ferraro MB, Martella F. Introduction to clustering: Springer; 2020.
- Borlea I-D, Precup R-E, Borlea A-B, Iercan D. A unified form of fuzzy C-means and K-means algorithms and its partitional implementation. Knowledge-Based Systems. 2021; 214: 106731.
- Mai Q, Zhang X, Pan Y, Deng K. A doubly enhanced em algorithm for model-based tensor clustering. Journal of the American Statistical Association. 2022; 117(540): 2120-34.
- Zangana HM, Abdulazeez AM. Developed Clustering Algorithms for Engineering Applications: A Review. International Journal of Informatics, Information System and Computer Engineering (INJIISCOM). 2023; 4(2): 147-69.
- Zhang M, editor Use density-based spatial clustering of applications with noise (DBSCAN) algorithm to identify galaxy cluster members. IOP conference series: earth and environmental science IOP Publishing. 2019.
- Cundari G, Marchitelli L, Pambianchi G, Catapano F, Conia L, Stancanelli G, et al. Imaging biomarkers in cardiac CT: moving beyond simple coronary anatomical assessment. La radiologia medica. 2024: 1-21.
- Maurovich-Horvat P, Ferencik M, Voros S, Merkely B, Hoffmann U. Comprehensive plaque assessment by coronary CT angiography. Nature Reviews Cardiology. 2014; 11(7): 390-402.
- Elnabawi YA, Dey AK, Goyal A, Groenendyk JW, Chung JH, Belur AD, et al. Coronary artery plaque characteristics and treatment with biologic therapy in severe psoriasis: results from a prospective observational study. Cardiovascular research. 2019; 115(4): 721-8.
- Aikawa E, Nahrendorf M, Figueiredo J-L, Swirski FK, Shtatland T, Kohler RH, et al. Osteogenesis associates with inflammation in early-stage atherosclerosis evaluated by molecular imaging in vivo. Circulation. 2007; 116(24): 2841-50.
- Kolossváry M, Karády J, Szilveszter B, Kitslaar P, Hoffmann U, Merkely B, et al. Radiomic features are superior to conventional quantitative computed tomographic metrics to identify coronary plaques with napkin-ring sign. Circulation: Cardiovascular Imaging. 2017; 10(12): 006843.
- Kolossváry M, Park J, Bang J-I, Zhang J, Lee JM, Paeng JC, et al. Identification of invasive and radionuclide imaging markers of coronary plaque vulnerability using radiomic analysis of coronary computed tomography angiography. European Heart Journal-Cardiovascular Imaging. 2019; 20(11): 1250-8.
- Kolossváry M, Karády J, Kikuchi Y, Ivanov A, Schlett CL, Lu MT, et al. Radiomics versus visual and histogram-based assessment to identify atheromatous lesions at coronary CT angiography: an ex vivo study. Radiology. 2019; 293(1): 89-96.
- Islam MM, Nipun SAA, Islam M, Rahat MAR, Miah J, Kayyum S, et al., editors. An Empirical Study to Predict Myocardial Infarction Using K-Means and Hierarchical Clustering. Machine Learning, Image Processing, Network Security and Data Sciences:Second International Conference, MIND. Proceedings, Part II 2; 2020: Springer. 2020; 30-31
- Seetharam K, Shrestha S, Sengupta PP. Artificial intelligence in cardiovascular medicine. Current treatment options in cardiovascular medicine. 2019; 21: 1-14.
- Prusty MR, Pandey TN, Lekha PS, Lellapalli G, Gupta A. Scalar invariant transform based deep learning framework for detecting heart failures using ECG signals. Scientific Reports. 2024; 14(1): 2633.
- Juarez-Orozco LE, Martinez-Manzanera O, Storti AE, Knuuti J. Machine learning in the evaluation of myocardial ischemia through nuclear cardiology. Current Cardiovascular Imaging Reports. 2019; 12: 1-8.
- Gomez J, Doukky R. Artificial intelligence in nuclear cardiology. Intelligence-Based Cardiology and Cardiac Surgery: Elsevier. 2024; 217-24.
- Nagamine T, Gillette B, Pakhomov A, Kahoun J, Mayer H, Burghaus R, et al. Multiscale classification of heart failure phenotypes by unsupervised clustering of unstructured electronic medical record data. Scientific Reports. 2020; 10(1): 21340.
- Carobene A, Campagner A, Uccheddu C, Banfi G, Vidali M, Cabitza F. The multicenter European Biological Variation Study (EuBIVAS): a new glance provided by the Principal Component Analysis (PCA), a machine learning unsupervised algorithms, based on the basic metabolic panel linked measurands. Clinical Chemistry and Laboratory Medicine (CCLM). 2022; 60(4): 556-68.
- He H, Tan Y, Xing J. Unsupervised classification of 12-lead ECG signals using wavelet tensor decomposition and two-dimensional Gaussian spectral clustering. Knowledge-Based Systems. 2019; 163: 392-403.
- Princy RJP, Parthasarathy S, Jose PSH, Lakshminarayanan AR, Jeganathan S, editors. Prediction of cardiac disease using supervised machine learning algorithms. 2020 4th international conference on intelligent computing and control systems (ICICCS); IEEE. 2020.
- Muhammad G, Naveed S, Nadeem L, Mahmood T, Khan AR, Amin Y, et al. Enhancing Prognosis Accuracy for Ischemic Cardiovascular Disease Using K Nearest Neighbor Algorithm: A Robust Approach. IEEE Access. 2023.
- Terrada O, Hamida S, Cherradi B, Raihani A, Bouattane O. Supervised machine learning based medical diagnosis support system for prediction of patients with heart disease. Advances in Science, Technology and Engineering Systems Journal. 2020; 5(5): 269-77.
- Patro SP, Padhy N, Chiranjevi D. Ambient assisted living predictive model for cardiovascular disease prediction using supervised learning. Evolutionary intelligence. 2021; 14(2): 941-69.
- Yu J, Taskén AA, Flade HM, Skogvoll E, Berg EAR, Grenne B, et al. Automatic assessment of left ventricular function for hemodynamic monitoring using artificial intelligence and transesophageal echocardiography. Journal of Clinical Monitoring and Computing. 2024: 1-11.
- Brown K, Roshanitabrizi P, Rwebembera J, Okello E, Beaton A, Linguraru MG, et al. Using Artificial Intelligence for Rheumatic Heart Disease Detection by Echocardiography: Focus on Mitral Regurgitation. Journal of the American Heart Association. 2024; 13(2): 031257.
- Föllmer B, Williams MC, Dey D, Arbab-Zadeh A, Maurovich-Horvat P, Volleberg RH, et al. Roadmap on the use of artificial intelligence for imaging of vulnerable atherosclerotic plaque in coronary arteries. Nature Reviews Cardiology. 2024; 21(1): 51-64.