Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
Stridor due to massive retrosternal goitre
*Corresponding Author : Eoin O’Connor*
Department of Anaesthesia, Connolly Hospital, Dublin, Ireland.
Tel: 08-58680666;
Email: eooconno@tcd.ie
Received : May 02, 2024
Accepted : May 20, 2024
Published : May 27, 2024
Archived : www.jcimcr.org
Copyright : © O’Connor E (2024).
Citation: O’Connor E. Stridor due to massive retrosternal goitre. J Clin Images Med Case Rep. 2024; 5(5): 3077.
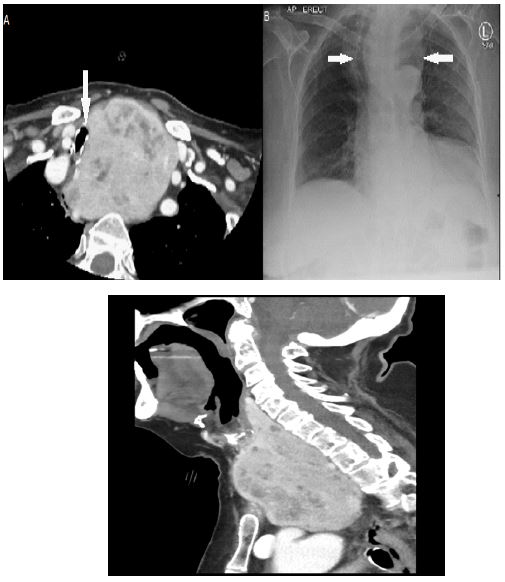
Description
An independent 90 year old woman presented to the emergency department in respiratory distress. Background medical history included a known retrosternal goitre under observation, previous right sided thyroid lobectomy and recent lower respiratory tract infection treated with oral antibiotics. The patient was tachypnoeic and ‘tripoding’. Stridor was immediately evident. Examination revealed tracheal tug and positive Pemberton’s sign. Radiological investigations included chest X-ray which showed tracheal deviation and a mediastinal mass. CT neck showed tracheal deviation and stenosis with minimum diameter of 0.6 cm at level of thoracic inlet, caused by massive retrosternal goitre. ABG revealed type 1 respiratory failure with PaO2 65 mmHg and PcO2 of 33 mmHg. PH was 7.47. Airway manoeuvres, intravenous steroid, nebulised epinephrine and bronchodilators had little to no beneficial effect. She was transferred urgently to a head and neck centre for consideration of emergency tracheal stenting.