
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 5
Cerebral manifestation of hypervirulent klebsiella pneumoniae: An in-depth case report on isolated brain abscess
Chun Chiuan Lee*; Nour Amalina Binti Mohd Said; Lee-Lee Low; Chou-Luan Tan
Internal Medicine Department, Hospital Sultanah Bahiyah, Malaysia.
*Corresponding Author : Chun Chiuan Lee
Internal Medicine Department, Hospital Sultanah Bahiyah, Malaysia
Email: chiuan_1993@hotmail.com
Received : May 17, 2024
Accepted : Jun 06, 2024
Published : Jun 13, 2024
Archived : www.jcimcr.org
Copyright : © Lee CC (2024).
Citation: Lee CC, Mohd Said NAB, Low LL, Tan CL. Cerebral manifestation of hypervirulent klebsiella pneumoniae: An in-depth case report on isolated brain abscess. J Clin Images Med Case Rep. 2024; 5(6): 3117
Introduction
Klebsiella pneumoniae (K. pneumoniae) is a gram negative organism commonly associated with respiratory tract infection. Isolated Invasive K. pneumoniae brain abscess and meningitis is extremely rare especially in an immunocompetent patient. There have been emerging cases of hypervirulent Klebsiella pneumoniae reported in Asia-Pacific [1]. These organisms have been associated with more invasive diseases, including meningitis, endophthalmitis, and liver abscesses. We are reporting a rare case of isolated hypervirulent Klebsiella pneumoniae brain abscess, with sterile blood cultures and no distance metastasis in an immunocompetent patient.
Case presentation
A 33-years old Malay gentleman presented with insidious onset of right sided unilateral weakness for 3 days with severe headache. He has type 2 diabetes mellitus and previous admissions with multiple admission due to localised Klebsiella pneumoniae perianal abscess which were adequately treated. On physical examination, his GCS was 15/15 and right sided hemiplegia (power 0/5).
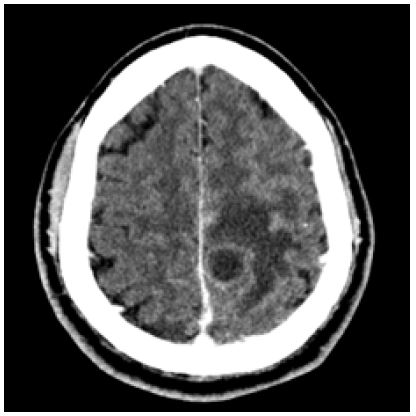
Contrast-Enhanced CT (CECT) Brain (Figure 1) revealed left fronto-parietal intra-axial hypodense lesion with ring enhancement, with increased meningeal enhancement at left fronto-parietal and right frontal region. Blood analysis showed elevated white cell counts predominantly neutrophils (72.2%), erythrocyte sedimentation rate (ESR; 94 mm/h) and glycated Haemoglobin A1c of 13.0%.
Lumbar puncture was performed; with opening pressure of 28 cm H20; Cerebrospinal fluid analysis revealed elevated protein (559 mg/L), increased white cell counts (364.9 cells/uL with predominant neutrophils) and reduced CSF/blood glucose ratio. However, CSF gram staining and cultures were negative. Human immunodeficiency virus, echocardiography, and blood culture were all unremarkable. Rest of the imaging does not revealed abscess in other systems.
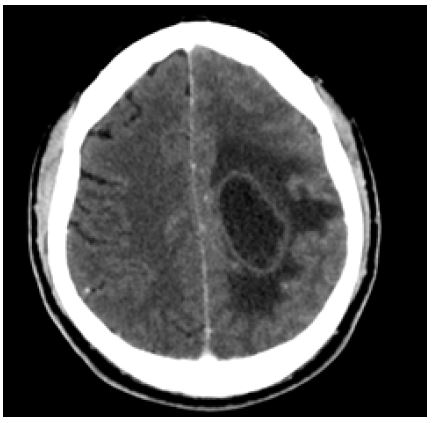
Patient was empirically treated with intravenous Ceftriaxone 2 g BD. However, patient condition deteriorated with worsening headache with persistent fever. Repeated CECT Brain (Figure 2) showed worsening mass effect and midline shift. He underwent emergency left craniotomy and excision of left parietal abscess. Intraoperatively, 20 ml pus with abscess capsule was removed. Intraoperative tissue, Cerebrospinal Fluid (CSF) and pus culture grew Klebsiella pneumoniae, sensitive to Cefuroxime, Augmentin, and Gentamicin. Further identification using conventional and molecular method revealed Hypervirulent Klebsiella pneumoniae, with positive String test, iroD, rmpA, peg gene and MagA gene detected.
He was treated with intravenous Ceftriaxone 2 g 12 hourly for a total of 8 weeks, optimization of blood glucose and in-patient rehabilitation, physiotherapy, and occupational therapy. He regained right sided power of 4/5 prior to discharge. Upon follow up in 3 months, he remained well and able to ambulate without aid with no recurrence.



Discussion
Klebsiella pneumoniae belongs to the Enterobacteriaceae family and is a gram negative, non-motile bacterium [2]. Primary reservoir for K. pneumoniae is human. In the general community, 5% to 38% of individuals carry the organism in their stool and 1% to 6% in the nasopharynx [3]. The main reservoir of infection are the patient’s gastrointestinal tract and the hands of hospital personnel [4].
Klebsiella pneumoniae associated with Community Acquired Pneumonia (CAP) mainly occurred in patient populations with alcohol use disorder or diabetes mellitus and common in Chinese ethnicity (reference). The isolation rates of K. pneumoniae from stool specimens in healthy adult Chinese was highest in Malaysia (87.7%), followed by Taiwan (75%), Singapore (61.1%) Hong Kong (58.8%) and China (57.9%) (reference). Pneumonia caused by K. pneumoniae is usually associated with high mortality, if not treated [3]. Overall, K. pneumoniae accounts for approximately 11.8% of all hospital-acquired pneumonia in the world. Mortality ranges from 50% to 100% in patients with alcoholism and septicaemia [1,3]. A study in Taiwan reported bacteremic CAP caused by K. pneumoniae in Taiwan from 2008 to 2013, accounting for 21.9% of all cases which are the commonest pathogen, with a high 30 day mortality of 54.1% [5].
Hypervirulent Klebsiella pneumoniae (hvKp) is an invasive variant that is more virulent than classical K. pneumoniae (cKp) with its hypermucoviscosity and hypervirulence characteristics [1,6]. This strain could be identified by the “string test,” using an inoculation instrument to create a sticky “string” of greater than 5 mm (Figure 7) [7]. HvKp infects individuals who are often healthy, unlikely cKp which infects old indivuals, however susceptible factors include diabetes mellitus, male gender, and Asian ethnicity, especially in Southeast Asia [7]. Due to hypervirulent characteristics, metastatic infections are very common, especially in the uncommon sites of infection such as pyogenic liver abscesses, necrotizing fasciitis, endophthalmitis, and meningitis. HvKp strains are commonly susceptible to a variety of antibiotics, including cephalosporins and carbapenem, except for its ampicillin resistance [6]. Thus, highly suspicious hvKp infected individuals such as Southeast Asian should undergone distance dissemination screening including imaging such as CECT Brain, CT Abdomen and ophthalmology referral.
An essential aspect of managing infectious diseases involves the identification and eradication of the source of K. pneumoniae, which presents a significant challenge. The need of source control such as drainage of abscesses/closed space infections is essential to obtain optimal outcome. Since hvKP strains often cause abscesses, interventional radiology and percutaneous drainage of accessible abscesses often needed in present era and rarely open surgical drainage is required in complicated cases [8]. As such in this case, isolated brain abscess can lead to elevated intracranial pressure and has significant morbidity and mortality and treatment of brain abscess has been a challenge. CT and MRI brain guides the management by localizing the abscess and offer details including the dimensions and number of abscesses. Surgical excision or drainage combined with prolonged antibiotics (usually 4-8 weeks) and weekly CT or MRI imaging able to obtain a cure rate of more than 90%, remains the treatment of choice for in brain abscess larger than 2.5 cm in diameter [10,11]. Steroid administration should be generally avoided unless the patient demonstrates signs of meningitis or disproportionate cytotoxic oedema and when used should be tapered as soon as possible [12].
Klebsiella Pneumoniae Invasive Syndrome (KPIS) is a rare clinical condition which characterised by liver abscesses with the following metastatic complications: bacteraemia, meningitis, endophthalmitis, and necrotising fasciitis. Early detection of hypervirulent strain eventually minimises the sequalae and improve clinical outcomes by early diagnosis and treatment. Patient’s condition become more critical and the mortality rate is higher when there is intracranial infection. CT examination of the head, chest and abdomen are recommended in the first instance and β-lactam antibiotics should be administered as soon as possible which hvKp is susceptible to it. For patients with this invasive syndrome, appropriate antimicrobial treatment combined with percutaneous drainage of liver abscesses increases their chances of survival [13].
Conclusion
Isolated Klebsiella pneumoniae brain abscess is a rare cause of community-acquired brain infection. Despite sterile CSF and blood cultures, a high index of suspicion is required to diagnose this rare entity, especially in a patient with invasive dissemination and risk factors. “String test” may be performed in laboratory to identify hypervirulent Klebsiella pneumoniae to aid in early identification of this pathogen. Treatment of K. pneumoniae brain abscess may include appropriate antibiotics and surgical evacuation if appropriate.
References
- Thomas A. Russo, Candace M. Hypervirulent Klebsiella pneumoniae. Marr 2019 May 15.
- John V. Ashurst; Adam Dawson. Klebsiella Pneumonia. 2023.
- Ren Chen, Shih-Neng Lin, Xin-Ni Wu, Sheng-Hua Chou, Fu-Der Wang, Yi-Tsung Lin. Clinical and Microbiological Characteristics of Bacteremic Pneumonia Caused by Klebsiella pneumoniae. 2023
- Yang CY, Lee CH, Hsieh CC, Ko WC, Lee CC. Etiology of Community-Onset Monomicrobial Bacteremic Pneumonia and Its Clinical Presentation and Outcome: Klebsiella and Pseudomonas Matters. 2017.
- Zhu, Tao Wang, Liang Chen, Hong Du. Virulence Factors in Hypervirulent Klebsiella pneumoniaeJie. 2021.
- Yi-Tsung Lin, L Kristopher Siu, Jung-Chung Lin, Te-Li Chen, Chih-Peng Tseng, Kuo-Ming Yeh, et al. Seroepidemiology of Klebsiella pneumoniae colonizing the intestinal tract of healthy chinese and overseas chinese adults in Asian countries.
- Performance characteristics and clinical predictive value of the string test for detection of hepato-virulent Klebsiella pneumoniae isolated from blood cultures. Thean Yen Tan, Yvonne Cheng, Melissa Ong, Lily Siew Yong Ng. 2013.
- Alyssa S. Shon, Rajinder PS. Bajwa, Thomas A. Russo. Hypervirulent (hypermucoviscous) Klebsiella pneumoniae A new and dangerous breed.
- De Chang, Lokesh Sharma, Charles S. Dela Cruz, Dong Zhang. 2021. Clinical Epidemiology, Risk Factors, and Control Strategies of Klebsiella pneumoniae Infection.
- Brain Abscess Maria R. Bokhari; Fassil B. Mesfin. 2022.
- Itzhak Brook. Microbiology and treatment of brain abscess.
- Dattatraya Muzumdar, Sukhdeep Jhawar, A. Goel. Brain abscess: An overview. 2011.
- L Kristopher Siu , Kuo-Ming Yeh, Jung-Chung Lin, Chang-Phone Fung, Feng-Yee Chang. Klebsiella pneumoniae liver abscess: a new invasive syndrome. 2012.