
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 5
A typical gastrointestinal metastasis of melanoma
Patrícia Moreira*; André Santos; Mafalda Vasconcelos; João Espírito Santo
Internal Medicine, Hospital Beatriz Ângelo, ULS Loures-Odivelas, Portugal.
*Corresponding Author : Patricia Moreira
Internal Medicine, Hospital Beatriz Ângelo, ULS
Loures-Odivelas, Portugal.
Tel: +351 916572982;
Email: anapatriciamoreira2@gmail.com
Received : Nov 01, 2024
Accepted : Nov 18, 2024
Published : Nov 25, 2024
Archived : www.jcimcr.org
Copyright : © Moreira P (2024).
Keywords: Metastatic; Melanoma; Anemia.
Citation: Moreira P, Santos A, Vasconcelos M, Santo JE. Atypical gastrointestinal metastasis of melanoma. J Clin Images Med Case Rep. 2024; 5(11): 3356.
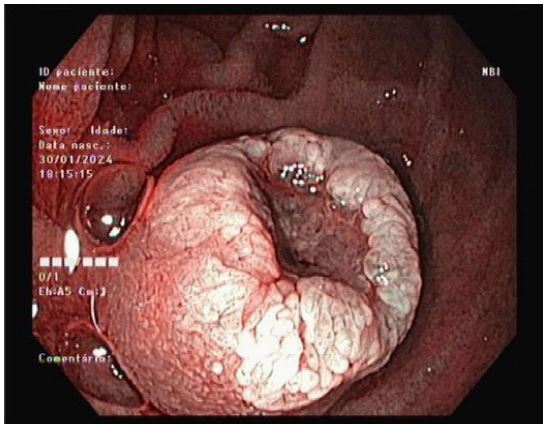
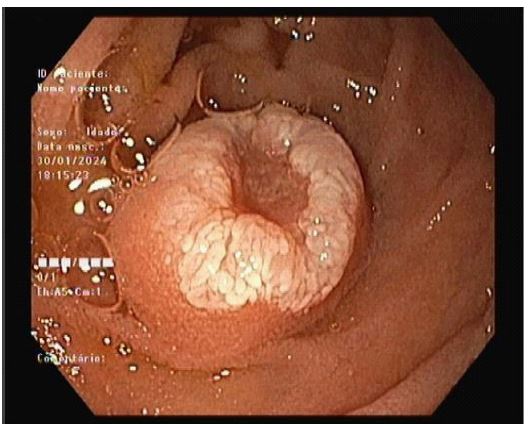
Description
A 74-year-old woman with a history of Charcot-Marie-Tooth type 1 neuropathy and malignant melanoma (TxN3bM0), diagnosed in 2023 and previously treated with pembrolizumab, presented to the emergency department with acute-on-chronic anemia (2 g/dL hemoglobin drop), heart failure, abdominal pain, hypotension, and melena. Endoscopic evaluation identified a highly infiltrative lesion at the junction of the duodenal bulb and second portion (D2) with a distinct “volcano-like” morphology. Histopathological examination confirmed the lesion as metastatic melanoma. Hemostatic radiotherapy was initiated, resulting in initial clinical improvement. However, the patient later became hemodynamically unstable, likely due to septic shock, and unfortunately passed away. Metastasis of melanoma to the gastrointestinal tract is well-documented but often underrecognized in clinical settings, as it typically remains asymptomatic until reaching advanced stages. Post-mortem studies reveal that 50-60% of patients with advanced melanoma show gastrointestinal involvement, though symptoms rarely present during life. This rarity in clinical presentation underscores the relevance of sharing these imaging findings [1].
References
- Kuykendall A, et al. Metastatic Patterns of Melanoma in the Era of Immune Checkpoint Inhibitors. Cancer Medicine. 2020; 9(14): 4662-4670.