
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
The use of 18F-Choline-PET/CT in chronic lymphocytic leukaemia
Ken Kudura1,2*; Beatrice Kern3; Martin HK Hoffmann1,2; Kwadwo Antwi1,2
1 Department of Radiology, St Clara Hospital AG, Basel, Switzerland.
2 Department of Nuclear Medicine, St Clara Hospital AG, Basel, Switzerland.
3 Department of Visceral Surgery, St Clara Hospital AG, Basel, Switzerland.
*Corresponding Author: Ken Kudura
Department of Radiology, Department of Nuclear
Medicine, St Clara Hospital AG, Basel, Switzerland.
Email: ken.kudura@claraspital.ch
Received : Mar 07, 2022
Accepted : Mar 29, 2022
Published : Apr 06, 2022
Archived : www.jcimcr.org
Copyright : © Kudura K (2022).
Citation: Kudura K, Kern B, Hoffmann MHK, Antwi K. The use of 18F-Choline-PET/CT in chronic lymphocytic leukaemia. J Clin Images Med Case Rep. 2022; 3(4): 1781.
Report
The use of 18F-2-Fluoro-2-Desoxy-D-Glucose Positron Emission Tomography/Computed Tomography (FDG-PET/CT) has become an integral part of patient management in many lymphoid malignancies. However, the diagnostic accuracy of FDG-PET/CT in some indolent lymphoid malignancies with commonly low FDG-avidity, including Chronic Lymphocytic Leukaemia (CLL) can still be challenging in clinical routine [1-3,6,9].
CLL is defined as a low-grade proliferative B-cell proliferative disease often indolent, which can in about 5% of the cases turn into a more aggressive malignancy, most commonly into Diffuse Large B-Cell Lymphoma (DLBCL). This transformation is called Richter transformation, often detected too late and associated with a poor prognosis. Therefore, accurate imaging of CLL at an early stage could be useful for the management of the disease and improve patient’ssurvival [4,5,7,8,10].
We report the case of a 76-years-old male patient with initial clinical symptoms of hyperparathyroidism. Initial blood samples were suspicious of primary hyperparathyroidism with the following results: Calcium 2.7 mmol/l, phosphate 0.7 mmol/l, parathormone 49.3 pg/ml as well as an increase excretion of calcium in urine.
An ultrasound of the thyroid and parathyroid glands was performed displaying a small (size 12 X 6 X 11 mm), ill-defined, hypoechogenic lesion posterior and cranial to the left thyroid lobe (Figure 1).

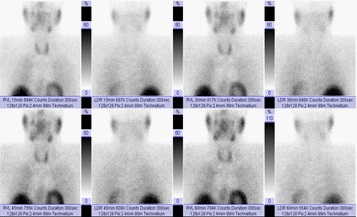
In suspicion of a parathyroid adenoma, scintigraphy using 99 m-Tc sestamibi (MIBI) with planar acquisitions and SinglePhoton Emission Tomography (SPECT/CT) of the parathyroid glands was carried out for localization diagnostics. This however proved negative with no evidence of increased tracer uptake in the thyroid glandorparathyroid glands (Figures 2,3).

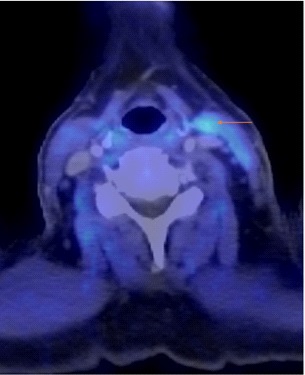
Following international recommendations in the case of a high clinical suspicion for a parathyroid adenoma, a 18F-fluorocholine-positron emission tomography/computerized tomography (F18-Choline PET/CT) was performed displaying a discrete tracer uptake cranial to left thyroid lobe (Figure 4).
Based on these findings, a parathyroidectomy was recommended and performed after patient consent. Intraoperatively, no enlarged parathyroid gland could be localized cranial to the left thyroid lobe but rather an enlarged cervical lymph node in the left cervical region inlevel III. The lymph node was excised and further investigated.
Histology of the resected left cervical level III lymph node cranial to the left thyroid lobe displayed an extensive infiltration of small cell lymphocytes population with the immunocytochemical expression of CD20, CD5 and some expression of CD23, corresponding to a B-CLL manifestation.
A literature search was performed in the PubMed database using the following keywords “choline” AND “PET” AND “leukaemia” or “CLL” with no results.
Conclusion
To the best of our knowledge, this case might be the first one to report the detection of a CLL manifestation using F18-Choline PET/CT. Given the commonly low FDG-avidity of CLL at an early stage on FDG-PET/CT scans and the risk of Richter transformation with poor prognosis further investigations on whether F18- CholinePET/CT can detect CLL manifestations should be considered.
References
- Alobthani, Galal, Victor Romanov, KayakoIsohashi, Keiko Matsunaga, et al. Value of 18F-FDG PET/CT in Discrimination between Indolent and Aggressive Non-Hodgkin’s Lymphoma: A Study of 328 Patients. Hellenic Journal of Nuclear Medicine. 2018; 21: 7–14. https://doi.org/10.1967/s002449910701.
- Cheson Bruce D, Richard I Fisher, Sally F Barrington, Franco Cavalli, Lawrence H, et al. Schwartz, Emanuele Zucca, T. Andrew Lister, u. A. Recommendations for Initial Evaluation, Staging, and Response Assessment of Hodgkin and Non-Hodgkin Lymphoma: The Lugano Classification. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology. 2014; 32: 3059–3068. https://doi.org/10.1200/JCO.2013.54.8800.
- El Galaly TC, D Villa, LC Gormsen, J Baech, ALo und CY Cheah, et al. FDG-PET/CT in the Management of Lymphomas: Current Status and Future Directions. Journal of Internal Medicine. 2018; 284: 358–376. https://doi.org/10.1111/joim.12813.
- Jain, Nitin, und Michael J. Keating. Richter Transformation of CLL. Expert Review of Hematology. 2016; 9: 793–801. https:// doi.org/10.1080/17474086.2016.1199948.
- Porrazzo, Marika, Emanuele Nicolai, Mara Riminucci, Candida Vitale, et al. Prognostic Significance of PET/CT in Patients with Chronic Lymphocytic Leukemia (CLL) Treated with Frontline Chemoimmunotherapy. Cancers. 2020; 12: E1773. https://doi. org/10.3390/cancers12071773.
- Schöder, Heiko, Ariela Noy, Mithat Gönen, Lijun Weng, et al. Intensity of 18 fluorodeoxyglucose Uptake in Positron Emission Tomography Distinguishes between Indolent and Aggressive Non-Hodgkin’s Lymphoma. Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology. 2005; 23: 4643–4651. https://doi.org/10.1200/JCO.2005.12.072.
- Shaikh, Faiq, AmnaJanjua, Frederick Van Gestel, und Adeel Ahmad. Richter Transformation of Chronic Lymphocytic Leukemia: A Review of Fluorodeoxyglucose Positron Emission Tomography-Computed Tomography and Molecular Diagnostics. Cureus. 2017; 9: e968. https://doi.org/10.7759/cureus.968.
- Tadmor, Tamar, und Ilana Levy. Richter Transformation in Chronic Lymphocytic Leukemia: Update in the Era of Novel Agents. Cancers. 2021; 13: 5141. https://doi.org/10.3390/cancers13205141.
- Wang, Danyang, YanleiHuo, Suyun Chen, Hui Wang, et al. Wholebody MRI versus 18F-FDG PET/CT for pretherapeutic assessment and staging of lymphoma: A meta-analysis. OncoTargets and therapy. 2018; 11: 3597–3608. https://doi.org/10.2147/ OTT.S148189.
- Yılmaz, Sabire, Meftune Özhan, Sertaç Asa, SaitSağer M, et al. Detection of Hodgkin Transformation in a Case of Chronic Lymphocytic Leukemia by PET/CT. Molecular Imaging and Radionuclide Therapy. 2014; 23: 67–69. https://doi.org/10.4274/ mirt.362.