
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Clinical Image - Open Access, Volume 3
Inflammatory myofibroblastic tumor: A rare case in the larynx
Joana Gonçalves*; Isa Elói; Nuno Silva; Ana Margarida Amorim; Jorge Miguéis
Department of Otolaryngology, Coimbra University Hospital Centre, Coimbra, Portugal.
*Corresponding Author: Joana Gonçalves
Department of Otolaryngology, Coimbra University Hospital Centre, Coimbra, Portugal.
Email: 11391@chuc.min-saude.pt
Received : Apr 11, 2022
Accepted : May 13, 2022
Published : May 20, 2022
Archived : www.jcimcr.org
Copyright : © Gonçalves J (2022).
Citation: Joana G, Isa E, Nuno S, Ana MA, Jorge M. Inflammatory Myofibroblastic Tumor: A rare case in the larynx. J Clin Images Med Case Rep. 2022; 3(5): 1843.
Case description
Inflammatory myofibroblastic tumors (IMTs) represent a heterogeneous group of mesenchymal benign neoplastic lesions, with a wide spectrum of histological presentations. IMT´s are most often located at the lungs. In the head and neck region, the most affected areas are the paranasal sinuses and orbits. Laryngeal involvement is extremely rare and occurs more frequently in the true vocal folds.
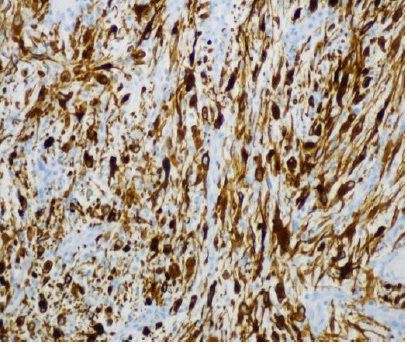
A 61-yer-old male presented with a 2-year history of progressive dyspnea. He never smoked and had no history of vocal abuse or gastroesophageal reflux. Laryngoscopy revealed an exophytic mass, with a smooth surface, located in the anterior commissure of the larynx (Figure 1). Cervical CT scan showed no signs of cartilage destruction or cervical lymph nodes. The mass was completely excised by suspension microlaryngoscopy with cold steel instruments. Histopathological analysis revealed spindle cells in a background of myxoid tissue and mixed inflammatory infiltrate. Immunohistochemistry was positive for vimentin, anaplastic lymphoma kinase (ALK)-1 and Caldesmon (Figure 2). The patient regained normal voice and remained asymptomatic during the 12-month follow-up.

Although benign, IMTs may have a more aggressive behavior with tissue destruction. Moreover, in the larynx these lesions represent a potential risk for acute dyspnea. For this reason, complete surgical resection is the treatment of choice for larynx IMTs. Follow-up is paramount to identify recurrence.
Declarations
Ethics approval and consent to participate: Not applicable.
Consent for publication: Written informed consent for publication of clinical details and clinical images was obtained from the patient.
Declaration of conflicting interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: There was no funding of this work.
References
- Guilemany JM, Alo L, Alobi I, Bernal-Sprekelsen M., Cardesa A. Inflammatory myofibroblastic tumor in the larynx: Clinicopathologic features and histogenesis. Acta OtoLaryngol, 2005; 125: 215-219.
- Sivesind T, Aderson A, Small J, Opperman D. Inflammatory Myofibroblastic Tumor of the Larynx: Report of a Case. J Voice. 2021; S0892-1997(21)00172-7.
- Izadi F, Ghanbari H, Azizi M, Gasembaglou S, Manteghi M, Ghanbari A. Iran J Otorhinolaryngol. 2016; 28(84): 79–82.