
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Short Report - Open Access, Volume 3
Urinary bladder hamartoma: A case of one of the rarest entities reported in urology
João Nuno Pereira1*; Andréia Bilé Silva2; João Vaz-Silva3; Ângelo Rodrigues3; Isaac Braga1
1Department of Urology, Portuguese Oncology Institute of Porto (IPO-Porto), Portugal.
2Department of Urology, Hospital Egaz Moniz, Centro Hospitalar de Lisboa Ocidental, Portugal.
3Department of Pathology, Portuguese Oncology Institute of Porto (IPO-Porto), Cancer Biology and Epigenetics Group, Research Center of IPO Porto (CI-IPOP), Portugal.
*Corresponding Author : João Nuno Pereira
Department of Urology, Portuguese Oncology Institute of Porto (IPO-Porto), Portugal.
Email: jnp.urologia@gmail.com
i2455@ipoporto.min-saude.pt
ORCID ID: 0000-0003-4627-5221
Received : Oct 25, 2022
Accepted : Nov 09, 2022
Published : Nov 16, 2022
Archived : www.jcimcr.org
Copyright : © Pereira JN (2022).
Abstract
Urinary Bladder Hamartoma (UBH) is one of the rarest entities reported in Urology, with, as far as we know, only fourteen cases reported in the literature. Otherwise, similar in presentation, imaging findings and macroscopic appearance as other bladder lesions, such as urothelial bladder carcinoma, UBH can solely be distinguished by histopathological examination. Therefore, we report an additional case of this rare tumour and provide a brief review of the current literature.
Keywords: Bladder hamartoma; Bladder lesions.
Citation: Pereira JN, Silva AB, Silva JV, Rodrigues A, Braga I, et al. Urinary bladder hamartoma: A case of one of the rarest entities reported in urology. J Clin Images Med Case Rep. 2022; 3(11): 2159.
Introduction
Hamartoma is traditionally defined as a benign tumour-like malformation composed of aberrant disorganized growth of mature tissues, often present at birth, but that can also be acquired later in life. Although it may occur in any body site, Urinary Bladder Hamartoma (UBH) is extremely rare. The first case of UBH was reported in 1949 by Davis [1] and, ever since, only fourteen other cases (including our patient) have been reported, as an isolated entity, or as part of a hereditary syndrome, such as Peutz-Jeghers syndrome, Beckwith-Wiedemann syndrome, Goldenhar Syndrome or multiple hamartomatous syndrome, also known as Cowden disease [2,3].
Results
A 67-year-old man was referred to our clinic with an incidental finding in a urinary bladder Ultrasound (US) of an 8 mm polypoid lesion on the posterior bladder wall. The patient had no associated Lower Urinary Tract Symptoms (LUTS), nor suprapubic pain or macroscopic haematuria.
Past medical history was remarkable for a medial third esophageal squamous cell carcinoma, stage IV (TNM stage classification according to 7th Edition of the AJCC Cancer Staging), treated between 2013 and 2014 with external radiotherapy (58 Gy/32 fractions) plus 4 cycles of cisplatin and 5-fluorouracil and no evidence of recurrence to date. He was a heavy smoker of about 80 pack-year. His family history was unremarkable.
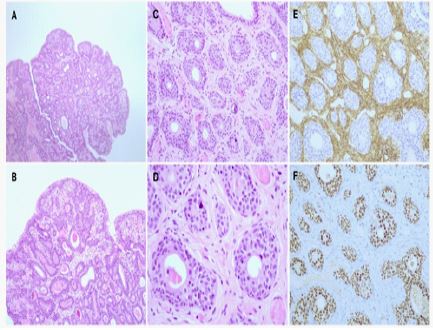
A physical examination did not show any contributory factor. Cystoscopic examination revealed a 1 cm polypoidal pedunculated lesion at the bladder neck. Patient underwent a Transurethral Resection of the Bladder Tumour (TURBT) lesion and the specimen was sent for histopathology. As the lesion macroscopically seemed a low-grade non-muscle invasive urothelial carcinoma, patient was given a single intravesical instillation of mitomycin 40 mg, two hours after surgery. Histopathological examination revealed, at low magnification, a polypoid lesion composed of crowded nests, resembling invaginated urothelial nests. The stromal component was composed of thin elongated spindle-shaped cells, which show immunoreactivity for Smooth-Muscle Actin (SMA), thus confirming the presence of a surrounding muscular stroma. At high magnification, both epithelial and stromal components presented bland cytologic features. Epithelial component displays positivity for GATA3 immunostaining (Figure 1).
After 12 months of follow-up, patient remains asymptomatic and no recurrence was recorded on cystoscopy.
Discussion
In all reported cases, UBH presents as a solitary lesion, ranging between 3 mm and 9 cm. Most of the cases are diagnosed in the context LUTS, gross haematuria or suprapubic pain. In this regard, our patient was the first case reported as an incidental finding in an otherwise asymptomatic adult [2,3]. Therefore, this presentation is not in agreement with solely proposed pathophysiology by Davis, that postulated that UBH may be a result of a chronic inflammatory process [1]. Those lesions are usually diagnosed by conventional radiological exams, such as urinary bladder US or pelvic Computed Tomography (CT), or by cystoscopy. Macroscopically, UBH cannot be distinguished from other bladder lesions and, in our specific case, it mimicked a small urothelial bladder carcinoma. For that reason, only pathologic examination enables a definitive diagnosis. Although the optimal management of UBH is not established due to the rarity of these lesions, in our understanding, the initial approach should be the same as the adopted for other bladder suspicious lesions, namely, a TURBT, if manageable endoscopically, or, if not, solely a biopsy, for a future more radical procedure, such as partial cystectomy.
All the reported cases had a benign behaviour, including invasive hamartomas, and no recurrences was seen in isolated UBH, although the surveillance described were not superior of five years [2,3]. For this reason, although cystoscopy should be the method of choice for surveillance, there is no agreement regarding the schedule and time of follow-up, with some authors advocating that cystoscopy should be performed every three months for a year and then yearly for four years or simply a long-term periodic cystoscopy as surveillance for recurrence. In our case, surveillance was performed with cystoscopy at 3 months, and then, at one year, and no signs of recurrence were noted [2,3].
Conclusion
Urinary bladder hamartoma is a very rare reported bladder lesion with a presentation undistinguishablefrom other bladder tumours, such as, urothelial carcinoma of the bladder. In this regard, the initial management should be a TURBT, in order to obtain a histopathological diagnosis and, if completely resectable, to cure the patient, as no recurrence was reported so far in isolated UBH. Given the sparse experience with UBH, no validated follow-up protocol can be advised. Therefore, surveillance should be based on cystoscopy, even though no specific schedule exists.
Declarations
Conflicts of interest: The authors declare that there are no conflicts of interest.
Fundings: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
References
- Davis TA. Hamartoma of the urinary bladder. Northwest Med. 1949; 48: 182-185.
- Al Shahwani N, Alnaimi AR, Ammar A, Al-Ahdal EM. Hamartoma of the urinary bladder in a 15-year-old boy. Turk J Urol. 2016; 42: 101-103.
- Kumar J, Albeerdy MI, Shaikh NA, et al. Bladder hamartoma in Peutz-Jeghers syndrome: A rare case report. Afr J Urol. 2021; 27: 74. https://doi.org/10.1186/s12301-021-00172-8.