
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 3
A malignancy mimicker in an unusual location:
Pseudotumoral malakoplakia of the breast
Mansouri Nada1; Rahma Yaiche1*; Gargouri Faten1; Felhi Fethi2; Tlili Karima1; Msakni Issam1; Laabidi Besma1
1Pathology Department, Military Hospital of Tunis, Montfleury 1008, Tunis, Tunisia.
2Department of Radiology, Military Hospital of Tunis, Montfleury, 1008, Tunis, Tunisia.
*Corresponding Author : Rahma Yaiche
Pathology Department, Military Hospital of Tunis, Montfleury, 1008, Tunis, Tunisia.
Phone: (+216) 22 653 878;
Email: rama.yae88@gmail.com
ORCID ID: 0000-0002-3635-0825
Received : Nov 11, 2022
Accepted : Dec 08, 2022
Published : Dec 15, 2022
Archived : www.jcimcr.org
Copyright : © Yaiche R (2022).
Abstract
Malakoplakia is an uncommon granulomatous disease that occurs in immunocompromised individuals. It’s thought to be caused by macrophagic bactericidal defect.
We report a rare case of breast malakoplakia in a pregnant 35 years-old woman that mimicked malignancy.
Pathological examination showed a circomscribed lesion of the breast parenchyma composed of an infiltrate of foamy histiocytes that had Michaelis and Gutmann PAS positive bodies in their cytoplasm. Malakoplakia occurs mainly in the genito-urinary tract, especially in the bladder.
Medical treatment is the standard treatment modality. Surgical treatment depends on affected site and is recommended and in case of medical treatment failure.
In conclusion, BM is very rare and may mimick malignancy leading to excessive mutilant treatment and psychologic complications. It should be managed by an interprofessional team approach since no clear treatment guidelines are established.
Keywords: Malakoplakia; Infection; Breast; Pathology; Mammography.
Citation: Nada M, Yaiche R, Faten G, Fethi F, Karima T, et al. A malignancy mimicker in an unusual location: Pseudotumoral malakoplakia of the breast. J Clin Images Med Case Rep. 2022; 3(12): 2200.
Introduction
Malakoplakia is an uncommon, granulomatous disease that occurs in immunocompromised individuals. It’s thought to be caused by a defect in macrophages functioning against bacterial agents. Breast is extremely rare as a site of occurrence [1].
We report the case of Breast Malakoplakia (BM) in a 35-year-old pregnant woman, that mimicked a malignant tumour and we aim to discuss its clinicopathological characteristics in this uncommon location.
Case report
The patient was a 35-year-old pregnant woman who presented with a nodule of the right breast. This nodule was discovered incidentally on a PT-scan performed to explore respiratory problems at the time of SARS-COV2 pandemics. The patients had a negative SARS-COV2 PCR and CT-Scan didn’t show any SARS-COV2 associated lesions. At clinical examination, the nodule was not palpable.
Mammography X-rays showed a speculated lesion that measured 8 mm in size. This suspicious aspect was confirmed by ultrasounds. Microbiopsies have been performed.
Pathological examination revealed a circumscribed lesion of the breast parenchyma. It was composed of an infiltrate of inflammatory cells within a myxoïd background. The predominant component of this inflammatory infiltrate was represented by a large number of foamy histiocytes with granular cytoplasm. These PAS positive granules are Michaelis and Gutmann bodies. In view of these histological aspects, we concluded to “breast pseudotumoral malakoplakia”.
The patient was put on fluoroquinolones (ciprofloxacin 500 mg, twice a day) with satisfying clinical and radiological evolution after 3 months.
Discussion
Historical aspects and terminology
Malkoplakiaor Von Hannsemman disease has been originally decribed in the early 1900s by Michaelis and Gutmann [2]. The name Malakoplakia has been attributed to this condition by Hannsemman, in 1903, from the Greek malakos (soft) and plakos (plaque) that represents its clinical aspect: Friable soft plaques [3].
Etiology and pathophysiology
Malakoplakia typically affects immunocompromised individuals. Its etiology is poorly understood.
It’s thought to be caused by macrophagic bactericidal defect. In fact, deficiencies in beta-glucuronidase and intracellular cGMP lead to impaired phagolysosomal activity and the accumulation of partially digested bacteria in macrophages, recognized microscopically as Michaelis-Gutmann bodies.
Organisms implicated in malakoplakia are gram-negative rods and Escherichia Coli is the most common organism associated with this condition.
Less frequent associations are with Klebsielle, Pseudomonas, Proteus, Enterococcus, Mycobacterium and Salmonelle [3-6].
Localization
Malakoplakia occurs mainly in the genito-urinary tract, especially in the bladder [7]. Other localizations may be seen like the skin, gastro-intestinal tract, lungs…
The first extra-urinary localization has been described in 1983 [8].
Breast localization is extremely rare. Few studies have reported Breast Malakoplakia (BM). In our knowledge, our case is the sixth described in the literature [9-12].
Other granulomatous lesions of the breast have been described but in these cases no particular investigations have been performed to confirm or rule out malakoplakia [13,14].
Epidemiology:
The peak incidence of malakoplakia is in patients over fifty [7].
In our case, the patient was 35 years old. BM has also been described in young female adults in two italian case reports [9,10]. In El Kataibi case report, the patient was 52 years-old [11].
In the urinary tract, there is a female predilection with a female to male sex ratio of 4:1. However, there is no gender prepredilection in extra-urinary localizations [1].
In the breast, it seems to be a female predominance of malakoplakia since in all the published cases of breast malakoplakia and in our case, the patient was a female.
Patient predisposition
In the literature, it is established that malakoplakia occurs mainly in immunocompromised individuals [15]. Repeated infection should raise suspicion of immunodeficiency.
In the two Italian reports of Di Léo [9,10], BM was related to the puerperal period. In our case, it was a pregnant woman. This can be explained by the weakened immune system during pregnancy and puerperal period.
Clinical presentation
Clinical presentation of malakoplakia differs according to the localization.
In the skin, all spectrums of lesions may be seen such as nodules, ulceration, papules.
In internal organs, it often presents as a mass or nodule [1].
In the breast, malakoplakia manifests itself frequently as a diffuse mastitis. In El Kataibi report [11] as in our case, the lesion presented as a breast nodule suspicious of malignancy without associated pseudoneoplastic mastitis.
In this same report of El Kataibi [11], the “orange skin” aspect and ulceration raised suspicion of malignancy.
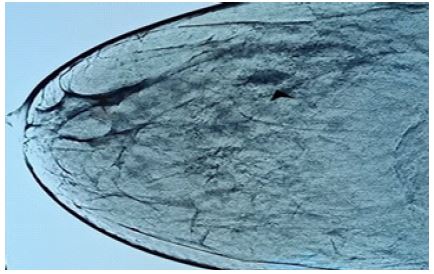
In our case, in which the nodule was discovered incidentally, radiologic aspects as spicules and poorly-defined edges were suspicious of malignancy (Figure 1).
Diagnosis
Histological examination is the main diagnosis tool. Malakoplakia can be self-limited or diffuse.
Its histological features don’t differ according to the localization.
Three stages are described: an initial inflammatory stage, a classic stage with abundant Michaelis-Gutmann bodies and a latest stage with progressive fibrous tissue and scarring.
The lesion is composed of foamy epithelioid histiocytes with PAS+ granular eosinophilic cytoplasm. These granules are Michaelis - Gutmann bodies which can be mineralized [15].
It’s important to explore the entire speciman to rule out any associated malignancy.
In our case (Figures 2 & 3), the limitation of the lesion and the use of PAS stain allowed to diagnose a benign lesion and not to report an «inadequacy» of the sample.
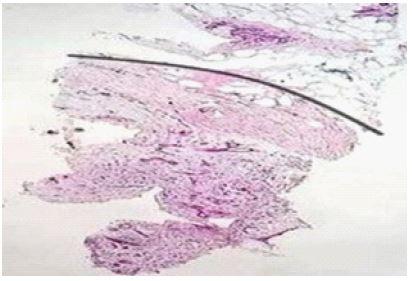

For this purpose, pathologists should be careful in examining inflammatory granulomatous lesions and rule out malakoplakia in order to prevent mutilant treatment while considering the absence of a malignant component of a suspicious mammographic lesion as a «non diagnostic» in the breast biopsy sample.
Although BM may be suspicious of malignancy clinically and radiologically, one should keep in mind these cancer mimickers. A well conducted questioning of the patient looking for infectious history, as well as a history of immunosuppressor treatment or of repeated infections may help diagnose this lesion early.
Managemen
There are no standardized treatment guidelines in malakoplakia. In fact, large clinical trials are lacking. Three treatment modalities may be applied including systemic antibiotic therapy, surgical excision and immunity boosting [1].
Medical treatment is the standard treatment modality. It is based on antibiotics such as fluoroquinolones, trimethoprim/sulfamethoxazole, and rifampin for a long period [1]. There is no standard for the duration of treatment.
Some studies have shown that decreasing or discontinuing Prednisone and Azathioprine in such situations allowed a recovery from malakoplakia [1].
Surgery depends on affected site and is recommended in case of medical treatment failure.
In case of aggressive lesions as it is mainly the case in the urinary system, a surgical treatment have to be considered [16-18].
In our case, the patient received antibiotic therapy by fluoroquinolones (ciprofloxacin 500 mg, twice a day) with ultrasonographic improvement after a 3 month-follow-up.
Prognosis
The outcome of malakoplakia depends on the localization, the extend of the lesion and, also on the immune status of the patient.
If not treated, malakoplakia may lead to chronic disease, but can rarely lead to death [19].
In breast location, a well-established diagnosis is necessary to avoid excessive mutilating treatment and psychological consequences.
Conclusion
In conclusion, Malakoplakia is a very rare granulomatous condition that typically occurs in immunocompromised individuals.
Breast location is seldom and may mimic malignancy, leading to excessive mutilating treatment and psychological complications.
BM should be managed by an interprofessional team approach since no clear treatment guidelines are established.
Large clinical trials should be conducted to best characterize therapeutic strategies.
Declarations
Acknowledgments: Author contributions: We would like to thank the staff of the department of pathology, radiology and gynaecology and obstetrics for their contributions in this work.
All authors have made substantial contributions in developing the research idea. All authors also declare that they have read and approved the final version of the manuscript:
MN: conceptualization and writing the presented idea/ YR: drafting the manuscript and submission/ GF: acquisition and analysis of data/ FF: providing imaging data/ TK: designing figures and writing captions/ MI, LB: supervision and verification of the final version of the manuscript.
Fundings: No funding was received to assist with the preparation of this manuscript.
Conflict of interest: The authors have no conflict of interest to declare.
Data availability statement: Data will be made available on request.
Ethical approval: This is an observational study. Research Ethics Committee of the military hospital of Tunis has confirmed that this work does not transgress ethics.
Consent statement: Written informed consent was obtained from the patient to publish this report in accordance with the journal’s patient consent policy.
References
- Kwan E, Riley CA, Robinson CA. Malakoplakia. [Updated 2021 Nov 5]. In: Stat Pearls [Internet]. Treasure Island (FL): Stat Pearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK564348/.
- Michaelis L, Gutmann C. Ubre Einschlusse in Blasentumore. Klin Med. 1902; 47: 208.
- Lowitt MH, Kariniemi AL, Niemi KM, utaneous malacoplakia: a report of two cases and review of the literature. J Am Acad Dermatol. 1996; 34: 325-332.
- Leão CA, Duarte MI, Gamba C, Malakoplakia after renal transplantation in the current era of immunosuppressive therapy: Case report and literature review. Transpl Infect Dis. 2012; 14: 137-141.
- Kohl SK, Hans CP. Cutaneous malakoplakia. Arch Pathol Lab Med. 2008; 132: 113-117.
- Tulpule MS, Bharatia PR, Pradhan AM, et al. Cutaneous malakoplakia: Interesting case report and review of literature. Indian J Dermatol Venereol Leprol. 2017; 83: 584-586.
- Long JP, Jr, Althausen AF. Malacoplakia: A 25-year experience with a review of the literature. J Urol. 1989; 141:1328–1331.
- Mc Clure J. Malakoplakia. J Pathol. 1983; 140: 275- 330.
- Tomasino RM, Ippolito R. Contributoallaconoscenza di lesionimammariepseudotumoraliomologabiliallamalacoplachia. Arch de Vecca Anatpatol. 1973; 59: 91–109.
- Di Leo S, Anastasi M. [Is there malacoplakia of the breast? Apropos of an unusual evolution of puerperal mastitis]. Arch De Vecchi Anat Patol. 1969; 55: 303-318. Italian.
- Elktaibi A, Elochi MR, Sinaa M, et al. Malakoplakiepseudotumorale du sein [Pseudotumoral malakoplakia of the breast]. Pan Afr Med J. 2015; 3; 21: 87. French.
- Bermejo M. Malacoplakia and Rosai-Dorfman disease: Two entities of histiocytic origin infrequently localized in the female breast-the cytologic aspect in aspirates obtained via fine-needle aspiration cytology. Diagn Cytopathol. 1993; 9: 698-704.
- Koo JS, Jung W. Xanthogranulomatous mastitis: Clinicopathology and pathological implications. Pathol Int. 2009; 59: 234-240.
- Bamanikar SA, Chandanwale SS, Pathak P, et al. A rare case of xanthogranulomatous mastitis with intraductal papilloma. Med J DY Patil Vidyapeeth. 2018; 11: 348-751.
- Roychowdhury M. Malakoplakia. Pathology Outlines. Com website. https://www.pathologyoutlines.com/topic/bladdermalakoplakia.html. Accessed June 6th, 2022.
- Cięszczyk K, Puderecki M, Wronecki L, Malakoplakia of the urinary system. Folia Med Cracov. 2019; 59: 67-74.
- Véan der Voort HJ, Ten Velden JA, Wassenaar RP, et al. Malacoplakia. Two case reports and a comparison of treatment modalities based on a literature review. Arch Intern Med. 199; 156: 577-583.
- Stanton MJ, Maxted W. Malacoplakia: A study of the literature and current concepts of pathogenesis, diagnosis and treatment. J Urol. 1981; 125: 139-146.
- Long JP, Althausen AF. Malacoplakia: A 25-year experience with a review of the literature. J Urol. 1989; 141: 1328-1331.