
Journal of Clinical Images and Medical Case Reports
ISSN 2766-7820
Case Report - Open Access, Volume 4
Occult type Ib endoleak not identified on imaging study as a cause of sac expansion refractory to treatment for recurrent type II endoleak
Kwon Cheol Yoo1,2*; Taeseung Lee3,4
1,2Department of Surgery, Chungbuk National University Hospital, Chunbuk National University, Chungdae-ro Seowon-gu, Cheongju, Chungbuk 28644, Korea.
3Department of Surgery, Seoul National University Bundang Hospital,Seongnam, Korea 82, Gumi-ro 173 Beon-gil, Bundang-gu, Gyeonggi-do 13620, Republic of Korea.
4Department of Surgery, Seoul National University College of Medicine, Seoul, Korea.
*Corresponding Author : Kwon Cheol Yoo
Department of Surgery, Chungbuk National University Hospital, Chunbuk National University, Chungdae-ro Seowon-gu, Cheongju, Chungbuk 28644, Korea.
Email: ykc1019@naver.com
Received : Jan 16, 2023
Accepted : Feb 03, 2023
Published : Feb 10, 2023
Archived : www.jcimcr.org
Copyright : © Yoo KC (2023).
Abstract
We report a case of serial occurrence of different type II endoleak from inferior mesenteric artery and lumbar artery. Despite repeated interventions, gradually expanding aneurysmal sac was eventually followed by impending rupture. In the end, the patient required open repair that revealed the type Ib endoleak which is not identified in CT scan or ultrasonography previously. The patient has been without any specific findings for 5 years without recurrence.
Citation: Yoo KC, Lee T. Occult type Ib endoleak not identified on imaging study as a cause of sac expansion refractory to treatment for recurrent type II endoleak. J Clin Images Med Case Rep. 2023; 4(2): 2280.
Introduction
As the management of abdominal aortic aneurysm advanced, Endo Vascular Aneurysm Repair (EVAR) has become popular since its introduction in 1986 [1-3]. It has benefit of less invasive, short hospital stay over open repair [4]. The major randomized control trials comparing open and endovascular repair of abdominal aortic aneurysm presented a remarkable benefit of endovascular repair with 30-day operative mortality [5-7]. However, endograft related complications, such as endo leak and migration following EVAR, require long-term surveillance due to the risk presented from the DREAM trial [8]. Endo leak significantly could cause post-EVAR rupture and patient death [9]. Thus, post-EVAR long-term surveillance of endoleak has become obligatory. We report a case of sequential occurrence of type II endoleak from inferior mesenteric artery and lumbar artery. Repetitive embolization of several causes could not prevent sac growing. Unsuspected endoleak in preoperative evaluation was identified in operative field and open repair was performed successfully.
Case report
A 67-year old man with a history of abdominal mass with pulsation since 5 years ago had increment of size of abdominal aortic aneurysm in CT scan. He had infra-renal type of aortic aneurysm with aneurysm of right common iliac artery. The maximal sac size of aneurysm had increased from 3.2 cm in 2007 to 5.7 cm in 2012. The proximal neck was 21 mm in diameter and 28 mm in length with angulation. He had been implanted with a Zenith bifurcated endograft (Cook Inc, Bloomington, Ind) and had right internal iliac artery embolization. Final angiography showed no significant endoleak from right internal iliac artery and other arteries.
The CT scan in POD 3 weeks showed focal contrast extravasation outside the stent, and it was doubt of endoleak; type II or type III. As there had not been any increment of sac size, close observation was done.
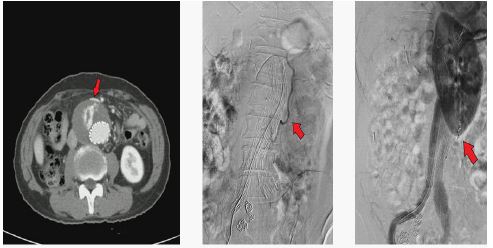
Every 6 months, patient had been checked with CT scan, and the size of aneurysmal sac had increased from 5.6 cm in Oct 2012 to 6.5 cm in Sep 2014. Due to endoleak from inferior mesenteric artery (Figure 1a). Second operation was planned to emboli the inferior mesenteric artery. Coil embolization of inferior mesenteric artery was done through the superior mesenteric artery (Figure 1b). Final angiography of secondary operation showed no significant endoleak in aneurysmal sac (Figure 1c).
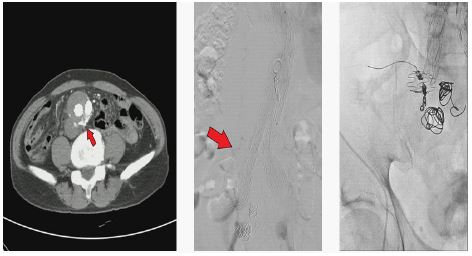
After the 6 months from secondary operation, follow up CT scan showed slight increment of aneurysmal sac from 6.5 cm to 6.7 cm. There had not been endoleak from inferior mesenteric artery due to coil embolization, but endoleak from lumbar artery was suspected. The size of sac had gradually grown from 7.5 cm in Oct 2016 to 8.5 cm in Apr 2017. The coil embolization of lumbar artery was planned to prevent sac growth in May 2017 (Figure 2).
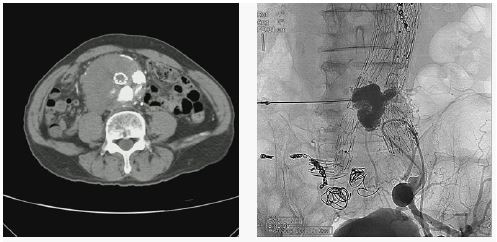
After the tertiary operation, he had been checked CT scan in other clinic. It showed the growth of sac and endoleak of type II and IV. The possibility of sac enlargement by stent graft endo-tension could not be ruled out. So, Aorto-uniiliac EVAR (Left), embolization of the right limb was done with Aplatzer Vascular plug and Femoral-femoral artery bypass (Left to Right) was performed in Mar 9 2018. On the follow up CT, sustained endoleak of type II from lumbar artery was observed and direct puncture embolization to lumbar artery was done in Jun 01, 2018 (Figure 3). Follow up CT scan from 6 months after 4th operation showed increment of sac size from 8.5 cm to 10 cm due to the sustained endoleak. Eventually, he underwent open repair with removal of previous endograft. In operative findings, cross-clamping of infra-renal artery was impossible for severely enlarged aneurysmal sac, so we clamped the suprarenal artery. In the aneurysmal sac, there were multiple endoleak from lumbar artery and they were ligated with prolene 5-0.
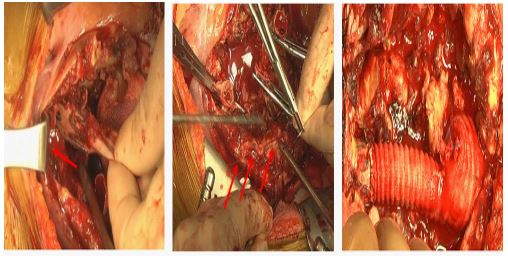
Interestingly, we could find occult type Ib of endoleak from right internal iliac artery which was occluded (Figure 4a) and unexpected several bleeders from arteriole of aneurysmal wall (Figure 4b) and, so it was ligated and closed with prolene 2-0. For bleeding control, reduction of aneurysmal wall was performed by using harmonic scalpel. We removed endo-graft except graft of left iliac limb and replace with Y-shaped PTFE graft which of right limb was resected and closed from infrarenal aorta to left iliac limb graft by end-to-end anastomosis (Figure 4c). On the color Doppler and ankle-brachial indexafter the operation, there were not abnormal findings including endoleak.
Discussion
Reduction of aneurysmal sac size is remarkable indication of the success of endograft treatment [10-13]. Mandatory post-EVAR surveillance is required to identify the aneurysmal sac and prevent the stent related complications.
Type II endoleak due to collateral flow of inferior mesenteric artery and lumbar artery showed benign progress which resolved spontaneously, whereas some experts consider it as a cause of late rupture [14]. First, type II endoleak alone is managed conservatively. Rarely, aneurysmal sac which has grown gradually after implantation of endograft requires embolization or ligation. In the presence of type II endoleak, there was observed in increment of sac size [15]. Although rupture due to the endoleak type II was uncommon and unpredictable, it shows the unclear indication when to intervene for prevent rupture [16]. As serial surveillance for enlargement of sac was prevent to rupture and determine the timing of intervention.
In our case, aneurysmal sac enlargement occurred with different types of endoleak that persisted in different time despite several attempts. Eventually, repair method had changed from endovascular to open. Repetitive different types of endoleak cause enlargement of aneurysmal sac, so it needs to repair with open methods. Moll and colleagues [17]. Recommended intervention with increased diameter of 10 mm or more, and open repair if endovascular repair fails (level II b).
The intervention for type II endoleak contains trans-arterial embolization with the aim of catheterizing the inferior mesentery artery or lumbar arteryand trans-lumbar embolization through the retroperitoneum. Type II endoleak was rarely treated with direct sac puncture and laparoscopic ligation. Aziz and colleagues [18] reported the incidence of persistent or recurrent endoleak after embolization was up to 74% in CT scan despite the intervention was judged to be successful.
Michael and colleagues [19] said that occult type I or III endoleak could hide the endoleak resolution itself, so suspicion of delayed or occult type I or III endoleak was recommended in the failure of repairing type II endoleaks and sac growth.
We recommend that the patient with persistent endoleak despite the single or repeated percutaneous endovascular treatment needs definitive treatment of the occult type II endoleak for contributing to the absence of aneurysm rupture and aneurysm-related mortality. Also, we have to doubt that unresolved aneurysmal sac could have other types of endoleak which was not observed in surveillance including ultrasonography or CT scan.
Conflict of interest: None.
References
- Volodos NL, Shekhanin VE, Karpovich IP, Troian VI, Gur’ev IuA, et al. A self-fixing synthetic blood vessel endoprosthesis. Vestn Khir Im I I Grek. 1986; 137: 123-125.
- Volodos NL, Karpovich IP, Troyan VI, Kalashnikova YuV, Shekhanin VE, et al. Clinical experience of the use of self-fixing synthetic prostheses for remote endoprosthetics of the thoracic and the abdominal aorta and iliac arteries through the femoral artery and as intraoperative endoprosthesis for aorta reconstruction. Vasa Suppl. 1991; 33: 93-95.
- Parodi J, Palmaz J, Barone H. Transfemoral intraluminal graft implantation for abdominal aortic aneurysms. Ann Vasc Surg. 1991; 5: 491-499.
- Greenhalgh RM, Brown LC, Kwong GP, Powell JT, Thompson SG, et al. Comparison of endovascular aneurysm repair with open repair in patients with abdominal aortic aneurysm (EVAR trial 1), 30-day operative mortality results: Randomised controlled trial. Lancet. 2004; 364: 843-848.
- EVAR Trial Participants, et al. Comparison of endovascular aneurysm repair with open repair in patients with abdominal aortic aneurysm (EVAR trial 1), 30-day operative mortality results: Randomized controlled trial. Lancet. 2004; 364: 843-848.
- Prinssen M, Verhoeven EL, Buth J. A randomized trial comparing conventional and endovascular repair of abdominal aortic aneurysms. N Engl J Med. 2004; 351: 1607-1618.
- Lederle FA, Freischlag JA, Kyriakides TC. Outcomes following endovascular vs open repair of abdominal aortic aneurysm: a randomized trial. JAMA. 2009; 302: 1535-1542.
- Blankensteijn J. Shocking and unexpected 5-year results from the DREAM trial. Veith Symposium; 2008; XIV.08
- Schlosser FJ, Gusberg RJ, Dardik A, Lin PH, Verhagen HJ, Moll FL, et al. Aneurysm rupture after EVAR: can the ultimate failure be predicted? Eur J Vasc Endovasc Surg. 2009; 37: 15e22
- Resch T, Ivancev K, Lindh M, Nyman U, Brunkwall J, Malina M, et al. Persistent collateral perfusion of abdominal aortic aneurysm does not lead to progressive change in aortic diameter. J Vasc Surg. 1998; 28: 242-249.
- Matsumura JS, Moore WS, for the Endovascular Technologies Investigators. Clinical consequences of peri-prosthetic leak after endovascular repair of abdominal aortic aneurysm. J Vasc Surg 1998; 27: 606-613.
- Resch T, Ivancev K, Brunkwall J, Nirhov N, Malina M, et al. Midterm changes in aortic aneurysm morphology after endovascular repair. J Endovasc Ther. 2000; 7: 279-285.
- Wolf YG, Hill BB, Rubin GD, Fogarty FJ, Zairns CK, et al. Rate of change of aneurysm diameter after endovascular repair. J Vasc Surg. 2000; 32: 108-115
- Wyss TR, Brown LC, Powell JT, Greenhalgh RM. Rate and predictability of graft rupture after endovascular and open abdominal aortic aneurysm repair: data from the EVAR trials. Ann Surg. 2010; 252: 805–812.
- Gould DA, McWilliams R, Edwards RD, Martin J, White D, et al. Aortic side branch embolisation before endovascular repair: incidence of type II endoleak. J Vasc Interv Radiol. 2001; 12: 337-341.
- Sidloff, DA, Stather PW, Choke E, Bown MJ, Sayers RD, et al. Type II endoleak after endovascular aneurysm repair. British Journal of Surgery. 100; 1262-1270.
- Moll FL, Powell JT, Fraedrich G, Verzini F, Haulon S, Waltham M. Management of abdominal aortic aneurysms clinical practice guidelines of the European society for vascular surgery. European journal of vascular and endovascular surgery. 2011; 41: S1-S58.
- Aziz A, Menias CO, Sanchez LA, Picus D, Saad N, et al. Outcomes of percutaneous endovascular intervention for type II endoleak with aneurysm expansion. Journal of vascular surgery. 2012; 55: 1263-1267.
- Madigan MC, Singh MJ, Chaer RA, Al-Khoury GE, Makaroun MS, et al. Occult type I or III endoleaks are a common cause of failure of type II endoleak treatment after endovascular aortic repair. Journal of vascular surgery. 2019; 69: 432-439.